

Rapid microbiological screening for tuberculosis in HIV-positive patients on the first day of acute hospital admission by systematic testing of urine samples using Xpert MTB/RIF: a prospective cohort in South Africa
- PMID: 26275908
- PMCID: PMC4537538
- DOI: 10.1186/s12916-015-0432-2
Rapid microbiological screening for tuberculosis in HIV-positive patients on the first day of acute hospital admission by systematic testing of urine samples using Xpert MTB/RIF: a prospective cohort in South Africa
Abstract
Background: Autopsy studies of HIV/AIDS-related hospital deaths in sub-Saharan Africa reveal frequent failure of pre-mortem diagnosis of tuberculosis (TB), which is found in 34-64 % of adult cadavers. We determined the overall prevalence and predictors of TB among consecutive unselected HIV-positive adults requiring acute hospital admission and the comparative diagnostic yield obtained by screening urine and sputum samples obtained on day 1 of admission with Xpert MTB/RIF (Xpert).
Methods: To determine overall TB prevalence accurately, comprehensive clinical sampling (sputum, urine, blood plus other relevant samples) was done and TB was defined by detection of Mycobacterium tuberculosis in any sample using Xpert and/or mycobacterial liquid culture. To evaluate a rapid screening strategy, we compared the diagnostic yield of Xpert testing sputum samples and urine samples obtained with assistance from a respiratory study nurse in the first 24 h of admission.
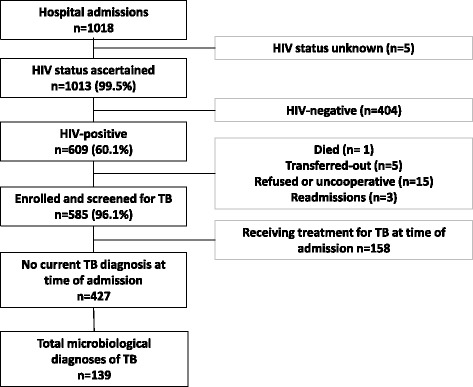
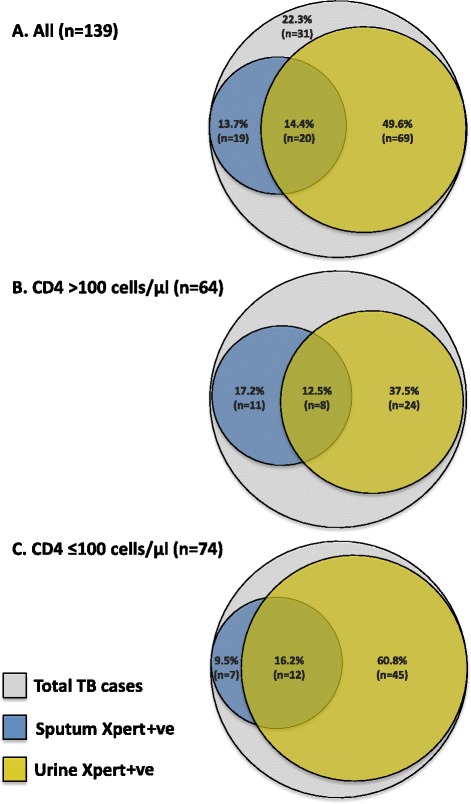
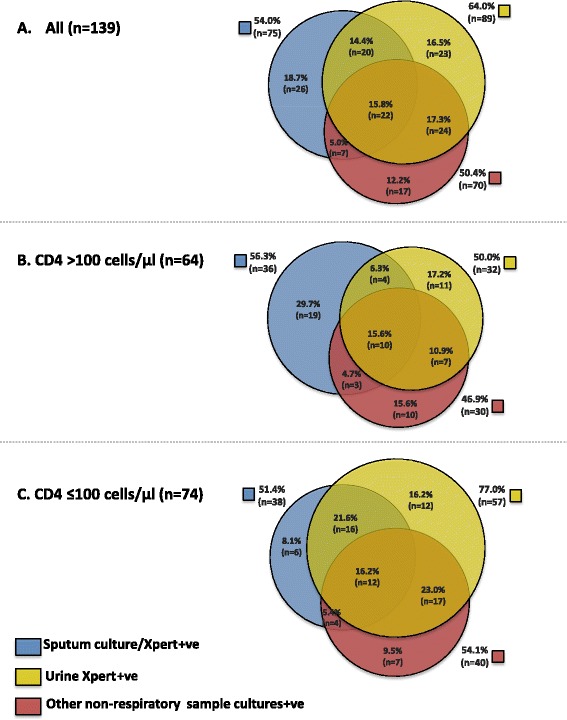
Results: Unselected HIV-positive acute adult new medical admissions (n = 427) who were not receiving TB treatment were enrolled irrespective of clinical presentation or symptom profile. From 2,391 cultures and Xpert tests done (mean, 5.6 tests/patient) on 1,745 samples (mean, 4.1 samples/patient), TB was diagnosed in 139 patients (median CD4 cell count, 80 cells/μL). TB prevalence was very high (32.6 %; 95 % CI, 28.1-37.2 %; 139/427). However, patient symptoms and risk factors were poorly predictive for TB. Overall, ≥1 non-respiratory sample(s) tested positive in 115/139 (83 %) of all TB cases, including positive blood cultures in 41/139 (29.5 %) of TB cases. In the first 24 h of admission, sputum (spot and/or induced samples) and urine were obtainable from 37.0 % and 99.5 % of patients, respectively (P <0.001). From these, the proportions of total TB cases (n = 139) that were diagnosed by Xpert testing sputum, urine or both sputum and urine combined within the first 24 h were 39/139 (28.1 %), 89/139 (64.0 %) and 108/139 (77.7 %) cases, respectively (P <0.001).
Conclusions: The very high prevalence of active TB and its non-specific presentation strongly suggest the need for routine microbiological screening for TB in all HIV-positive medical admissions in high-burden settings. The incremental diagnostic yield from Xpert testing urine was very high and this strategy might be used to rapidly screen new admissions, especially if sputum is difficult to obtain.
Figures
References
-
- World Health Organization (WHO). Global tuberculosis report 2014. Geneva: WHO; 2014. Available at: http://apps.who.int/iris/bitstream/10665/137094/1/9789241564809_eng.pdf?.... Accessed 31 July 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
