

Mobile Exercise Apps and Increased Leisure Time Exercise Activity: A Moderated Mediation Analysis of the Role of Self-Efficacy and Barriers
- PMID: 26276227
- PMCID: PMC4642397
- DOI: 10.2196/jmir.4142
Mobile Exercise Apps and Increased Leisure Time Exercise Activity: A Moderated Mediation Analysis of the Role of Self-Efficacy and Barriers
Abstract
Background: There are currently over 1000 exercise apps for mobile devices on the market. These apps employ a range of features, from tracking exercise activity to providing motivational messages. However, virtually nothing is known about whether exercise apps improve exercise levels and health outcomes and, if so, the mechanisms of these effects.
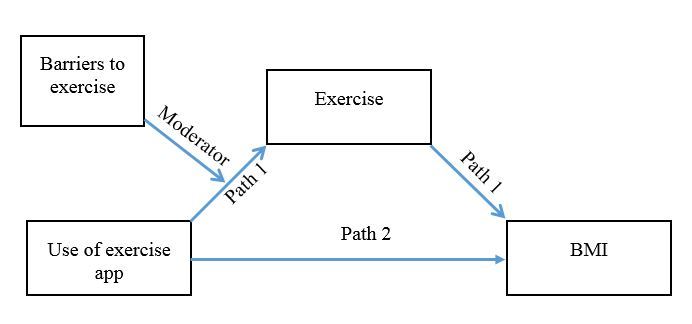
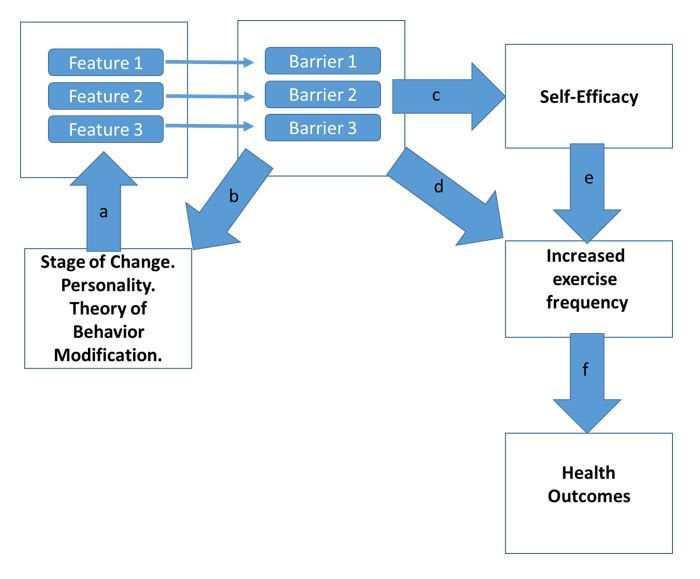
Objective: Our aim was to examine whether the use of exercise apps is associated with increased levels of exercise and improved health outcomes. We also develop a framework within which to understand how exercise apps may affect health and test multiple models of possible mechanisms of action and boundary conditions of these relationships. Within this framework, app use may increase physical activity by influencing variables such as self-efficacy and may help to overcome exercise barriers, leading to improved health outcomes such as lower body mass index (BMI).
Methods: In this study, 726 participants with one of three backgrounds were surveyed about their use of exercise apps and health: (1) those who never used exercise apps, (2) those who used exercise apps but discontinued use, and (3) those who are currently using exercise apps. Participants were asked about their long-term levels of exercise and about their levels of exercise during the previous week with the International Physical Activity Questionnaire (IPAQ).
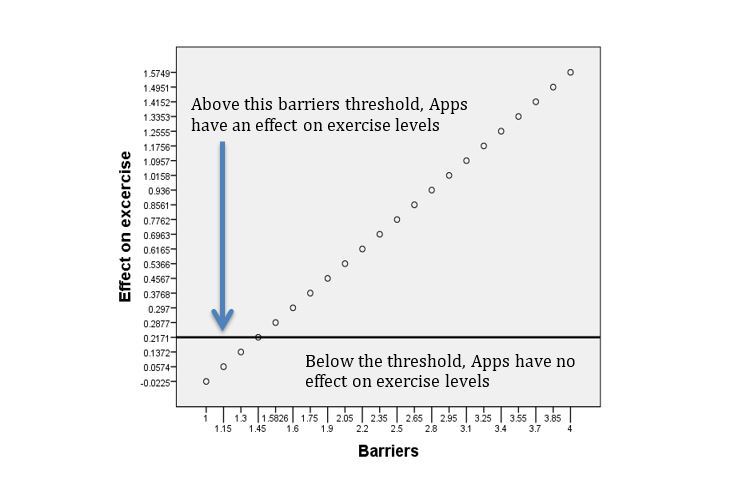
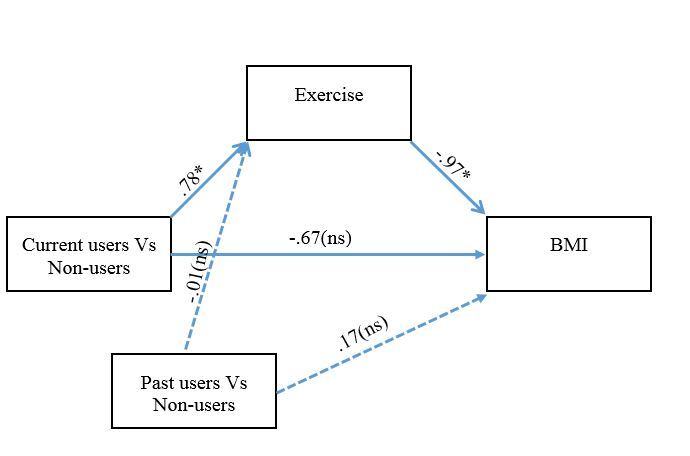
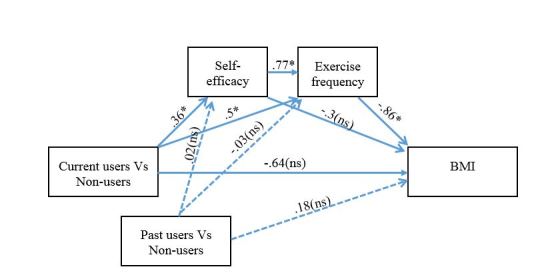
Results: Nearly three-quarters of current app users reported being more active compared to under half of non-users and past users. The IPAQ showed that current users had higher total leisure time metabolic equivalent of task (MET) expenditures (1169 METs), including walking and vigorous exercise, compared to those who stopped using their apps (612 METs) or who never used apps (577 METs). Importantly, physical activity levels in domains other than leisure time activity were similar across the groups. The results also showed that current users had lower BMI (25.16) than past users (26.8) and non-users (26.9) and that this association was mediated by exercise levels and self-efficacy. That relationship was also moderated by perceived barriers to exercise. Multiple serial mediation models were tested, which revealed that the association between app use and BMI is mediated by increased self-efficacy and increased exercise.
Conclusions: Exercise app users are more likely to exercise during their leisure time, compared to those who do not use exercise apps, essentially fulfilling the role that many of these apps were designed to accomplish. Data also suggest that one way that exercise apps may increase exercise levels and health outcomes such as BMI is by making it easier for users to overcome barriers to exercise, leading to increased self-efficacy. We discuss ways of improving the effectiveness of apps by incorporating theory-driven approaches. We conclude that exercise apps can be viewed as intervention delivery systems consisting of features that help users overcome specific barriers.
Keywords: BMI; apps; barriers to exercise; exercise; mobile health; self-efficacy.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Boulos Maged N Kamel, Wheeler S, Tavares C, Jones R. How smartphones are changing the face of mobile and participatory healthcare: an overview, with example from eCAALYX. Biomed Eng Online. 2011;10:24. doi: 10.1186/1475-925X-10-24. http://www.biomedcentral.com/1475-925X/10/24 1475-925X-10-24 - DOI - PMC - PubMed
-
- Fox S, Duggan M. Mobile Health. 2012. [2015-07-17]. http://www.pewinternet.org/2012/11/08/mobile-health-2012/
-
- Liu C, Zhu Q, Holroyd KA, Seng EK. Status and trends of mobile-health applications for iOS devices: A developer's perspective. Journal of Systems and Software. 2011 Nov;84(11):2022–2033. doi: 10.1016/j.jss.2011.06.049. - DOI
-
- Mosa Abu Saleh Mohammad, Yoo I, Sheets L. A systematic review of healthcare applications for smartphones. BMC Med Inform Decis Mak. 2012;12:67. doi: 10.1186/1472-6947-12-67. http://www.biomedcentral.com/1472-6947/12/67 1472-6947-12-67 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
