

Further Peripheral Vascular Dysfunction in Heart Failure Patients With a Continuous-Flow Left Ventricular Assist Device: The Role of Pulsatility
- PMID: 26277768
- PMCID: PMC4568148
- DOI: 10.1016/j.jchf.2015.04.012
Further Peripheral Vascular Dysfunction in Heart Failure Patients With a Continuous-Flow Left Ventricular Assist Device: The Role of Pulsatility
Abstract
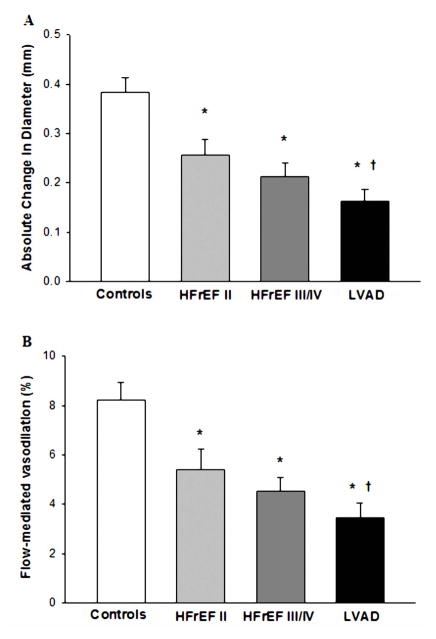
Objectives: Using flow-mediated vasodilation (FMD) and reactive hyperemia (RH), this study aimed to provide greater insight into left ventricular assist device (LVAD)-induced changes in peripheral vascular function.
Background: Peripheral endothelial function is recognized to be impaired in patients with heart failure with reduced ejection fraction (HFrEF), but the peripheral vascular effects of continuous-flow LVAD implantation, now used as either a bridge to transplantation or as a destination therapy, remain unclear.
Methods: Sixty-eight subjects (13 New York Heart Association [NYHA] functional class II HFrEF patients, 19 NYHA functional class III/IV HFrEF patients, 20 NYHA functional class III/IV HFrEF patients post-LVAD implantation, and 16 healthy age-matched control subjects) underwent FMD and RH testing in the brachial artery with blood flow velocity, artery diameters, and pulsatility index (PI) assessed by ultrasound Doppler.
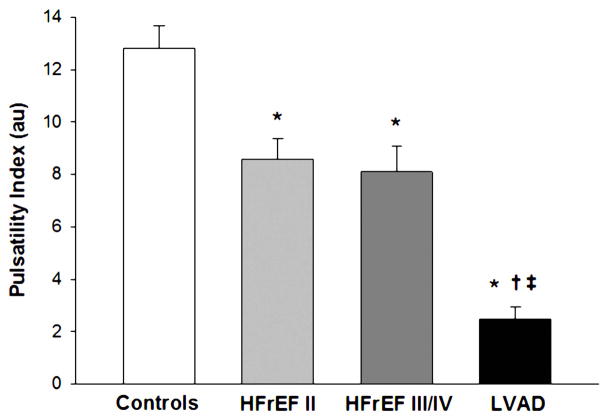
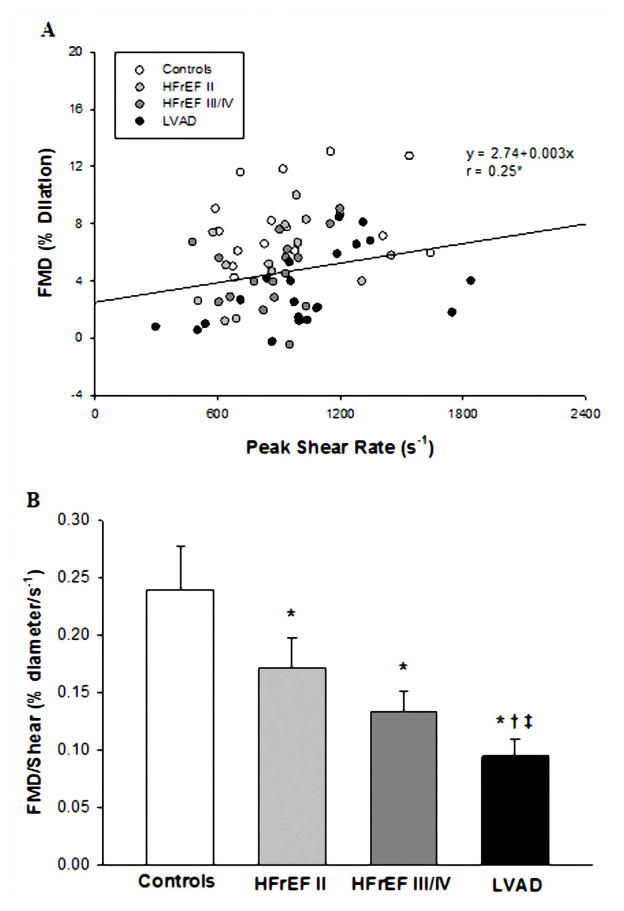
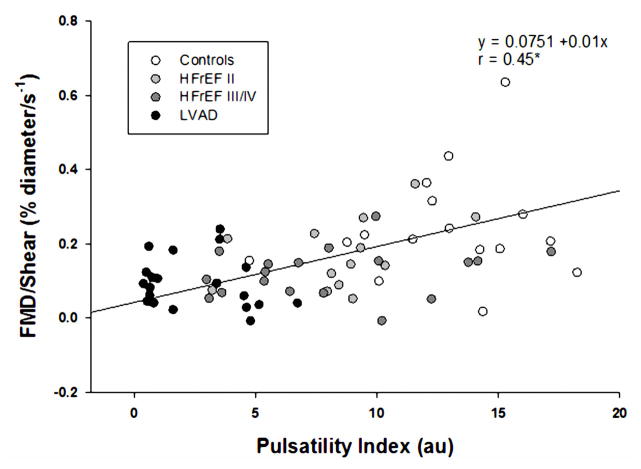
Results: PI was significantly lower in the LVAD group (2.0 ± 0.4) compared with both the HFrEF II (8.6 ± 0.8) and HFrEF III/IV (8.1 ± 0.9) patients, who, in turn, had significantly lower PI than the control subjects (12.8 ± 0.9). Likewise, LVAD %FMD/shear rate (0.09 ± 0.01 %Δ/s(-1)) was significantly reduced compared with all other groups (control subjects, 0.24 ± 0.03; HFrEF II, 0.17 ± 0.02; and HFrEF III/IV, 0.13 ± 0.02 %Δ/s(-1)), and %FMD/shear rate significantly correlated with PI (r = 0.45). RH was unremarkable across groups.
Conclusions: Although central hemodynamics are improved in patients with HFrEF by a continuous-flow LVAD, peripheral vascular function is further compromised, which is likely due, at least in part, to the reduction in pulsatility that is a characteristic of such a mechanical assist device.
Keywords: HFrEF; blood flow; flow-mediated vasodilation; mechanical assist; pulsatility.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Changing the Carburetor Without Changing the Plugs: The Intersection of Stock Car Racing With Mechanically Assisted Circulation.JACC Heart Fail. 2015 Sep;3(9):712-4. doi: 10.1016/j.jchf.2015.07.001. Epub 2015 Aug 12. JACC Heart Fail. 2015. PMID: 26277763 No abstract available.
Similar articles
-
Effects of Continuous-Flow Left Ventricular Assist Device Therapy on Peripheral Vascular Function.ASAIO J. 2022 Feb 1;68(2):214-219. doi: 10.1097/MAT.0000000000001447. ASAIO J. 2022. PMID: 35089263
-
Macrovascular and microvascular function after implantation of left ventricular assist devices in end-stage heart failure: Role of microparticles.J Heart Lung Transplant. 2015 Jul;34(7):921-32. doi: 10.1016/j.healun.2015.03.004. Epub 2015 Mar 24. J Heart Lung Transplant. 2015. PMID: 25980571
-
Vascular function in continuous-flow left ventricular assist device recipients: effect of a single pulsatility treatment session.Am J Physiol Regul Integr Comp Physiol. 2021 Apr 1;320(4):R425-R437. doi: 10.1152/ajpregu.00274.2020. Epub 2021 Jan 13. Am J Physiol Regul Integr Comp Physiol. 2021. PMID: 33438517 Free PMC article.
-
Endothelial Function in Patients With Continuous-Flow Left Ventricular Assist Devices.Angiology. 2021 Jan;72(1):9-15. doi: 10.1177/0003319720946977. Epub 2020 Aug 6. Angiology. 2021. PMID: 32757767 Review.
-
The Unique Blood Pressures and Pulsatility of LVAD Patients: Current Challenges and Future Opportunities.Curr Hypertens Rep. 2017 Oct 18;19(10):85. doi: 10.1007/s11906-017-0782-6. Curr Hypertens Rep. 2017. PMID: 29043581 Free PMC article. Review.
Cited by
-
Significant impact of left ventricular assist device models on the value of flow-mediated dilation: effects of LVAD on endothelial function.Heart Vessels. 2020 Feb;35(2):207-213. doi: 10.1007/s00380-019-01474-2. Epub 2019 Jul 20. Heart Vessels. 2020. PMID: 31327031
-
The study on hemodynamic effect of series type LVAD on aortic blood flow pattern: a primary numerical study.Biomed Eng Online. 2016 Dec 28;15(Suppl 2):163. doi: 10.1186/s12938-016-0252-4. Biomed Eng Online. 2016. PMID: 28155672 Free PMC article.
-
Vasoplegia from Continuous Flow Left Ventricular Assist Devices.Curr Cardiol Rep. 2021 Jul 1;23(8):101. doi: 10.1007/s11886-021-01534-y. Curr Cardiol Rep. 2021. PMID: 34196837 Review.
-
Changes in circulating stem cells and endothelial progenitor cells over a 12-month period after implantation of a continuous-flow left ventricular assist device.Arch Med Sci. 2020 Nov 2;16(6):1440-1443. doi: 10.5114/aoms.2020.100306. eCollection 2020. Arch Med Sci. 2020. PMID: 33224344 Free PMC article.
-
Approaches to improving exercise capacity in patients with left ventricular assist devices: an area requiring further investigation.Expert Rev Med Devices. 2019 Sep;16(9):787-798. doi: 10.1080/17434440.2019.1660643. Epub 2019 Sep 6. Expert Rev Med Devices. 2019. PMID: 31453716 Free PMC article. Review.
References
-
- Panza JA, Quyyumi AA, Brush JE, Jr, Epstein SE. Abnormal endothelium-dependent vascular relaxation in patients with essential hypertension. N Engl J Med. 1990;323:22–7. - PubMed
-
- Monnink SH, van Haelst PL, van Boven AJ, et al. Endothelial dysfunction in patients with coronary artery disease: a comparison of three frequently reported tests. J Investig Med. 2002;50:19–24. - PubMed
-
- Katz SD, Biasucci L, Sabba C, et al. Impaired endothelium-mediated vasodilation in the peripheral vasculature of patients with congestive heart failure. J Am Coll Cardiol. 1992;19:918–25. - PubMed
-
- Drexler H, Hayoz D, Munzel T, et al. Endothelial function in chronic congestive heart failure. Am J Cardiol. 1992;69:1596–601. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
