

Hypoplastic left heart syndrome is associated with structural and vascular placental abnormalities and leptin dysregulation
- PMID: 26278057
- PMCID: PMC4609616
- DOI: 10.1016/j.placenta.2015.08.003
Hypoplastic left heart syndrome is associated with structural and vascular placental abnormalities and leptin dysregulation
Abstract
Introduction: Hypoplastic left heart syndrome (HLHS) is a severe cardiovascular malformation (CVM) associated with fetal growth abnormalities. Genetic and environmental factors have been identified that contribute to pathogenesis, but the role of the placenta is unknown. The purpose of this study was to systematically examine the placenta in HLHS with and without growth abnormalities.
Methods: HLHS term singleton births were identified from a larger cohort when placenta tissue was available. Clinical data were collected from maternal and neonatal medical records, including anthropometrics and placental pathology reports. Placental tissues from cases and controls were analyzed to assess parenchymal morphology, vascular architecture and leptin signaling.
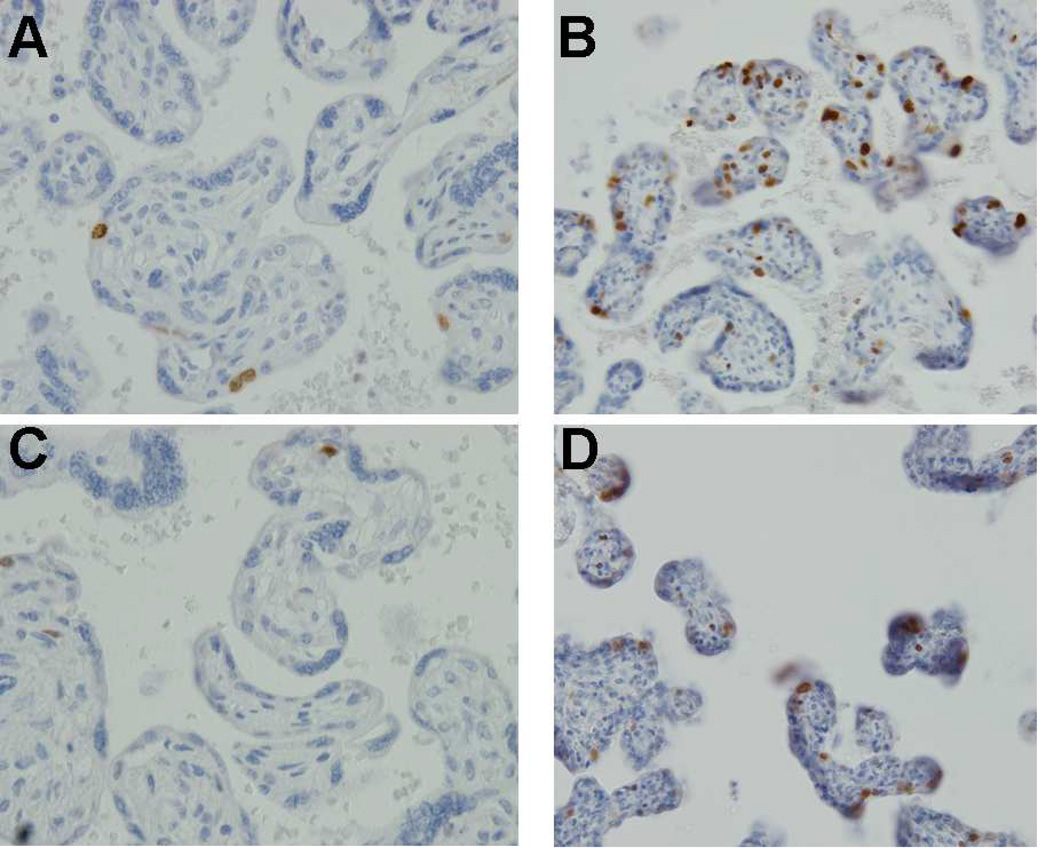
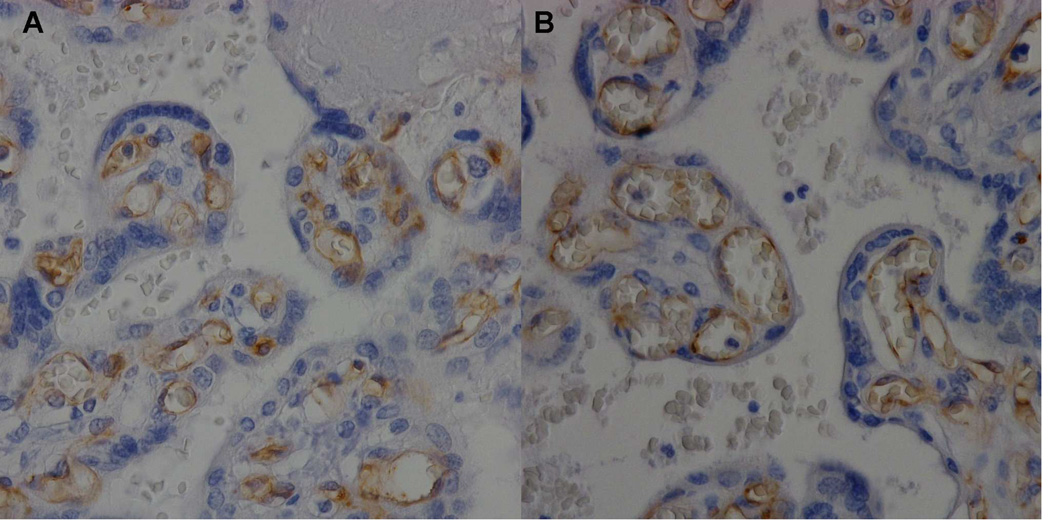
Results: HLHS cases (n = 16) and gestational age-matched controls (n = 18) were analyzed. Among cases, the average birth weight was 2993 g, including 31% that were small for gestational age. When compared with controls, gross pathology of HLHS cases demonstrated significantly reduced placental weight and increased fibrin deposition, while micropathology showed increased syncytial nuclear aggregates, decreased terminal villi, reduced vasculature and increased leptin expression in syncytiotrophoblast and endothelial cells.
Discussion: Placentas from pregnancies complicated by fetal HLHS are characterized by abnormal parenchymal morphology, suggesting immature structure may be due to vascular abnormalities. Increased leptin expression may indicate an attempt to compensate for these vascular abnormalities. Further investigation into the regulation of angiogenesis in the fetus and placenta may elucidate the causes of HLHS and associated growth abnormalities in some cases.
Keywords: Angiogenesis; Congenital heart disease; Vascular biology.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures





References
-
- Atz AM, Travison TG, Williams IA, Pearson GD, Laussen PC, Mahle WT, et al. Pediatric Heart Network Investigators. Prenatal diagnosis and risk factors for preoperative death in neonates with single right ventricle and systemic outflow obstruction: screening data from the Pediatric Heart Network Single Ventricle Reconstruction Trial(*) J Thorac Cardiovasc Surg. 2010;140:1245–1250. - PMC - PubMed
-
- Gaynor JW, Mahle WT, Cohen MI, Ittenbach RF, DeCampli WM, Steven JM, et al. Risk factors for mortality after the Norwood procedure. Eur J Cardiothorac Surg. 2002;22:82–89. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
