

Bench-to-bedside review: the effects of hyperoxia during critical illness
- PMID: 26278383
- PMCID: PMC4538738
- DOI: 10.1186/s13054-015-0996-4
Bench-to-bedside review: the effects of hyperoxia during critical illness
Abstract
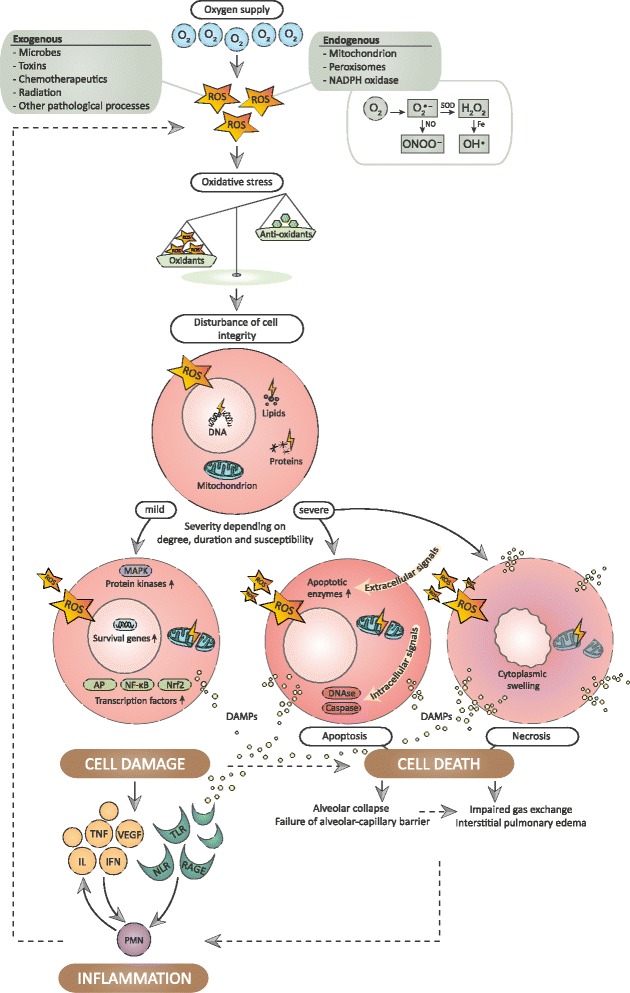
Oxygen administration is uniformly used in emergency and intensive care medicine and has life-saving potential in critical conditions. However, excessive oxygenation also has deleterious properties in various pathophysiological processes and consequently both clinical and translational studies investigating hyperoxia during critical illness have gained increasing interest. Reactive oxygen species are notorious by-products of hyperoxia and play a pivotal role in cell signaling pathways. The effects are diverse, but when the homeostatic balance is disturbed, reactive oxygen species typically conserve a vicious cycle of tissue injury, characterized by cell damage, cell death, and inflammation. The most prominent symptoms in the abundantly exposed lungs include tracheobronchitis, pulmonary edema, and respiratory failure. In addition, absorptive atelectasis results as a physiological phenomenon with increasing levels of inspiratory oxygen. Hyperoxia-induced vasoconstriction can be beneficial during vasodilatory shock, but hemodynamic changes may also impose risk when organ perfusion is impaired. In this context, oxygen may be recognized as a multifaceted agent, a modifiable risk factor, and a feasible target for intervention. Although most clinical outcomes are still under extensive investigation, careful titration of oxygen supply is warranted in order to secure adequate tissue oxygenation while preventing hyperoxic harm.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
