

The Functional Lumen Imaging Probe Detects Esophageal Contractility Not Observed With Manometry in Patients With Achalasia
- PMID: 26278501
- PMCID: PMC4663149
- DOI: 10.1053/j.gastro.2015.08.005
The Functional Lumen Imaging Probe Detects Esophageal Contractility Not Observed With Manometry in Patients With Achalasia
Abstract
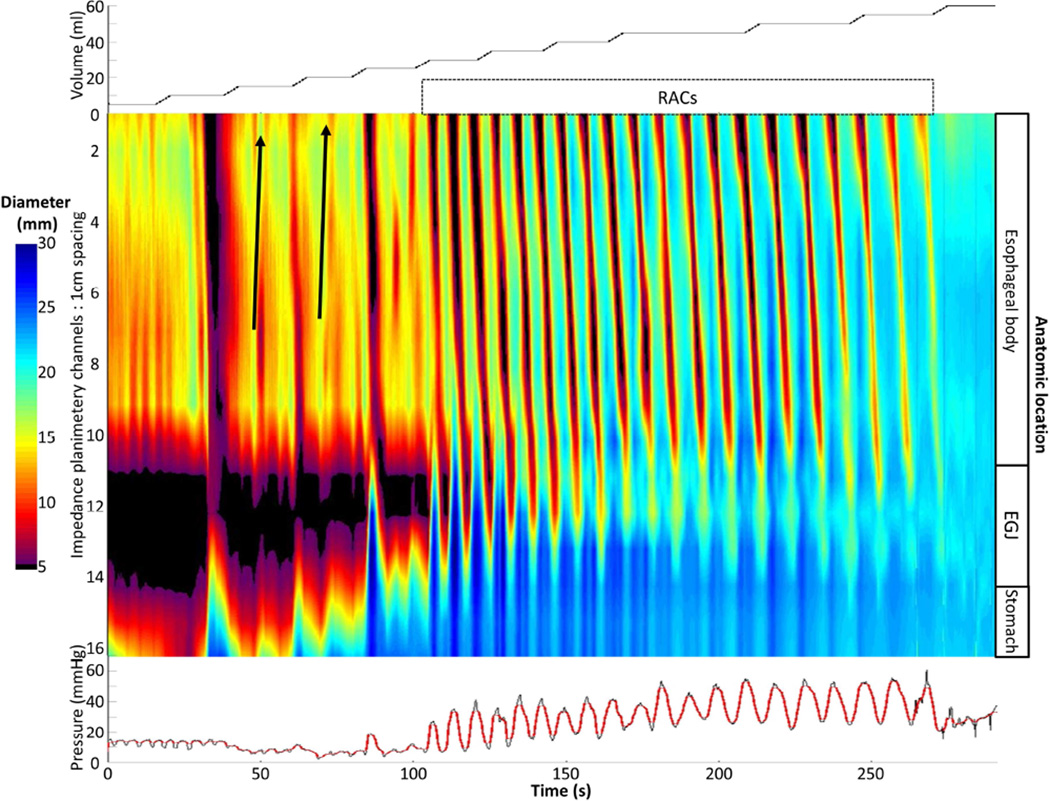
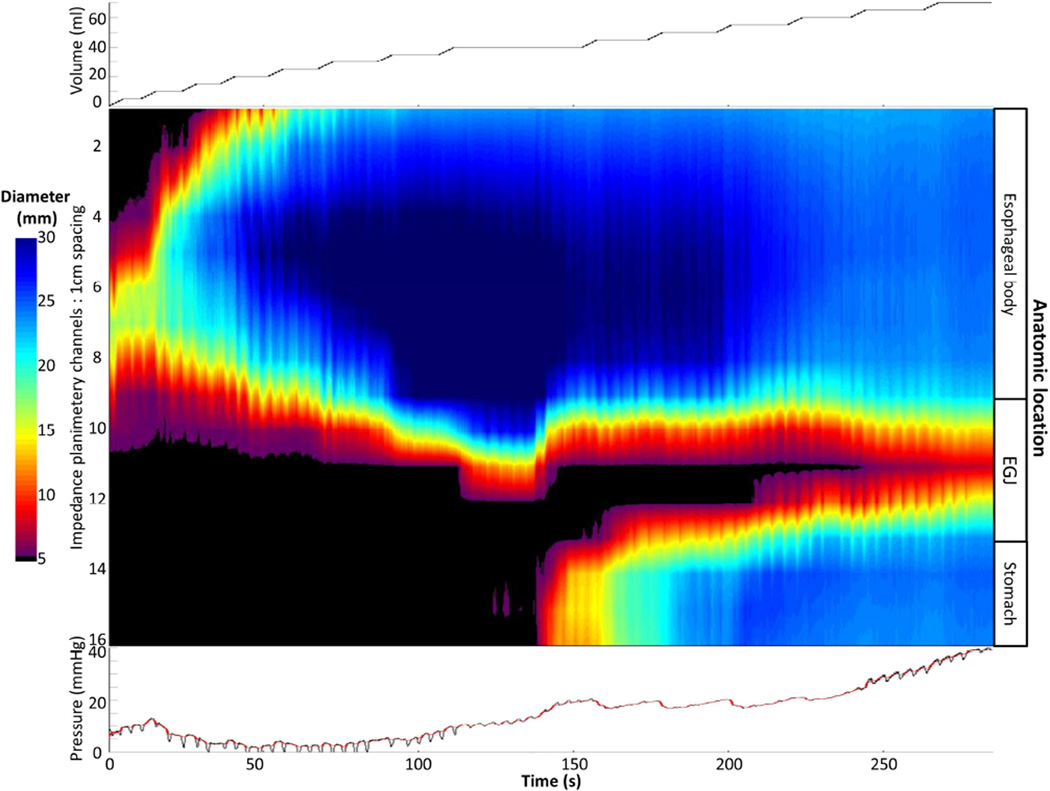
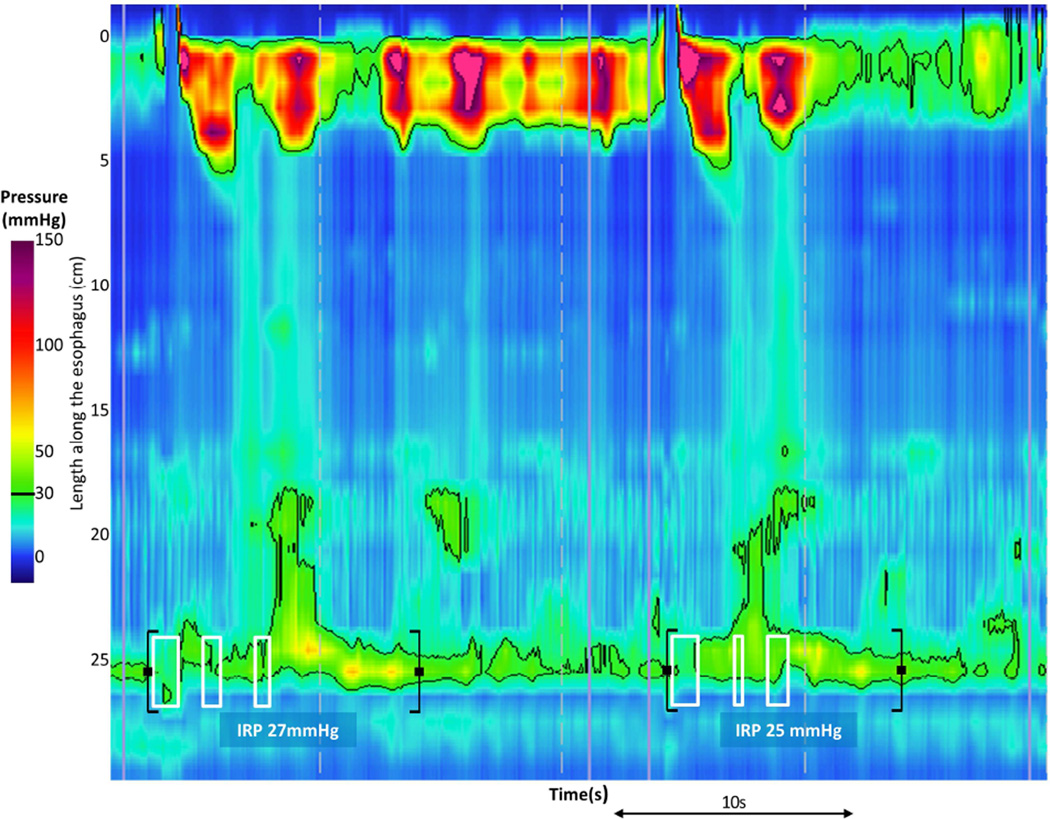
Background & aims: The functional lumen imaging probe (FLIP) could improve the characterization of achalasia subtypes by detecting nonocclusive esophageal contractions not observed with standard manometry. We aimed to evaluate esophageal contractions during volumetric distention in patients with achalasia using FLIP topography.
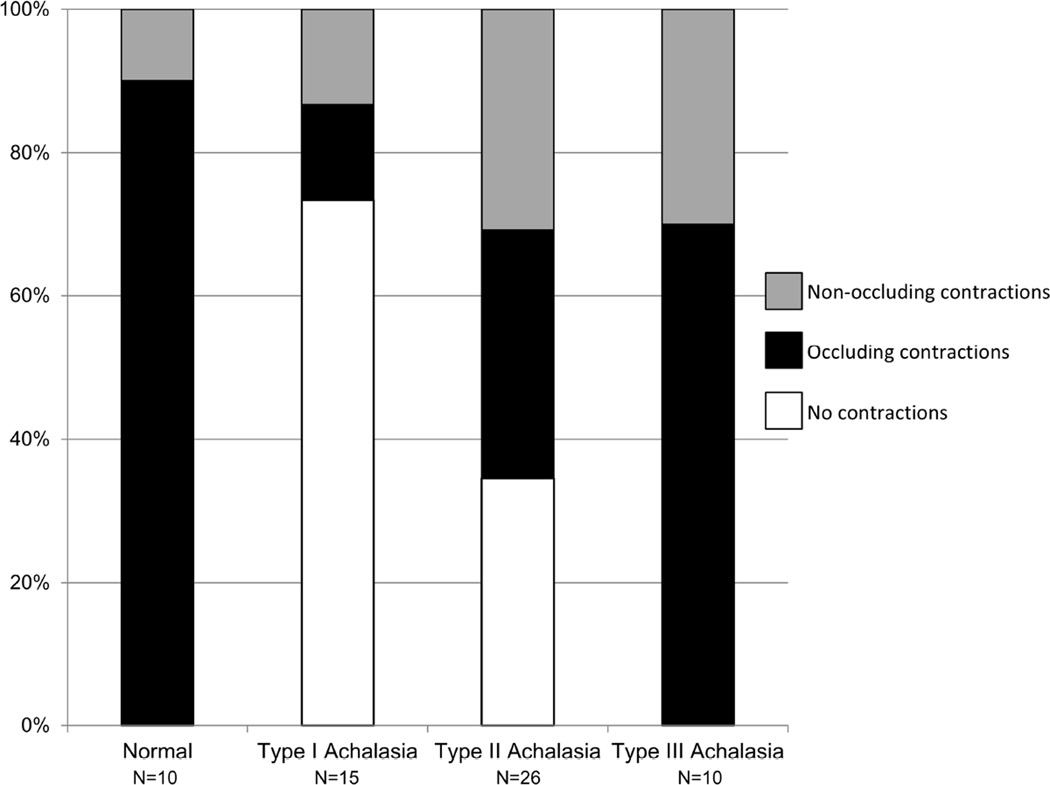
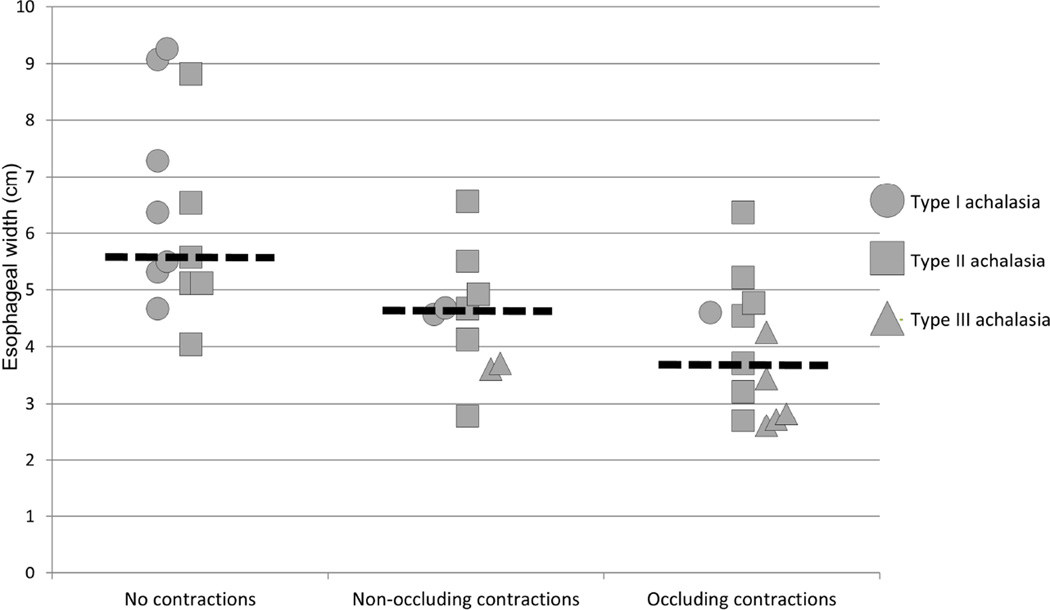
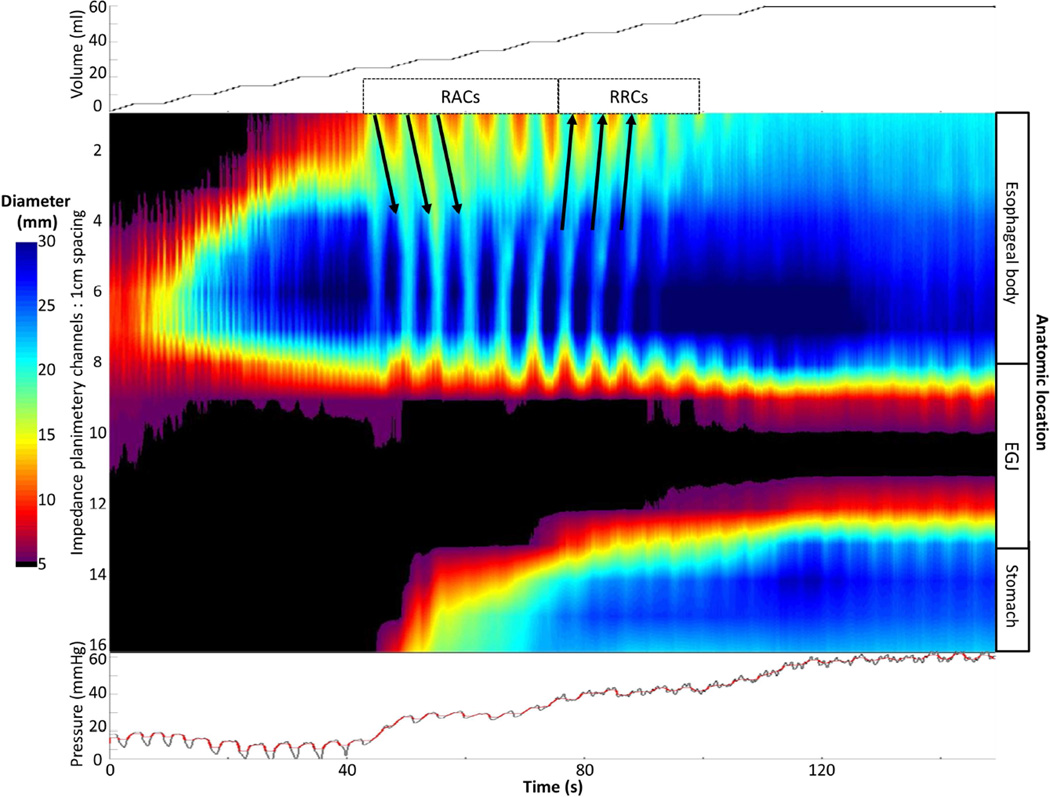
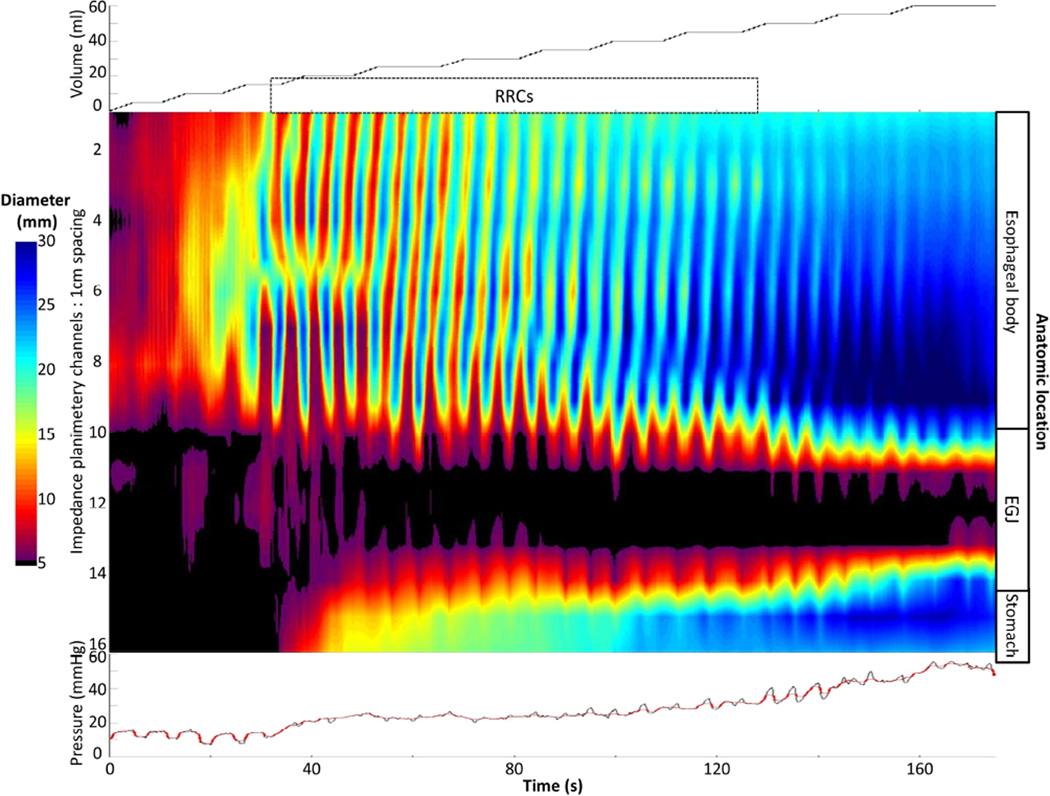
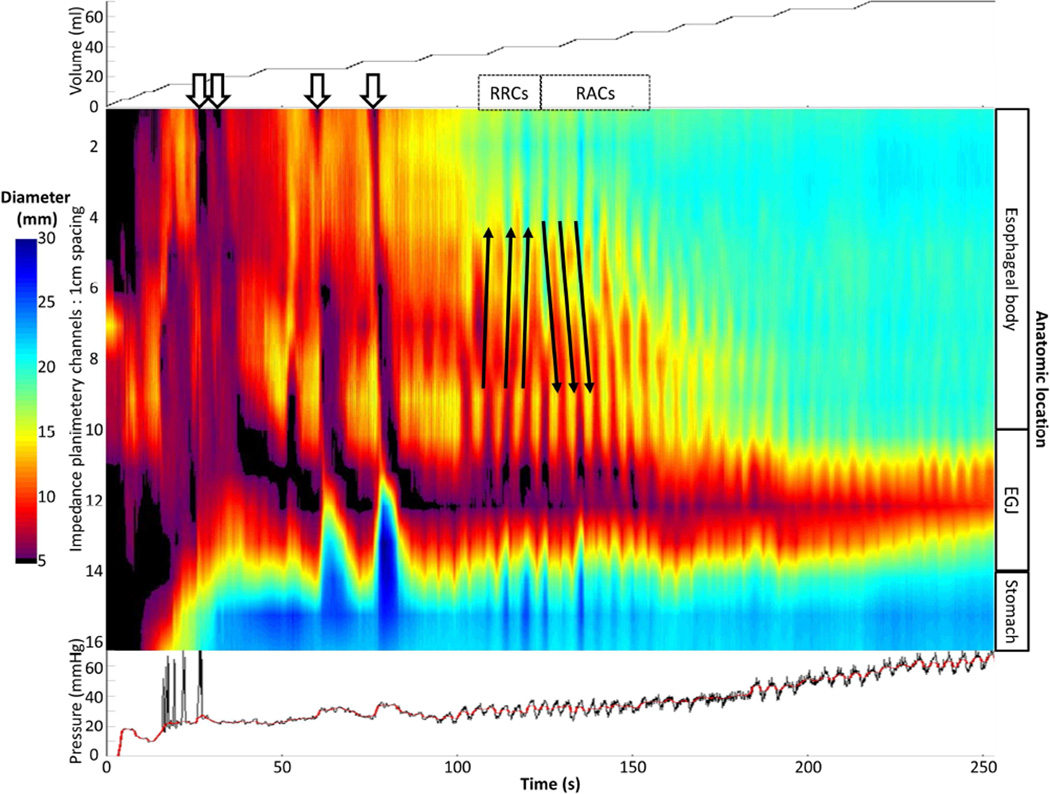
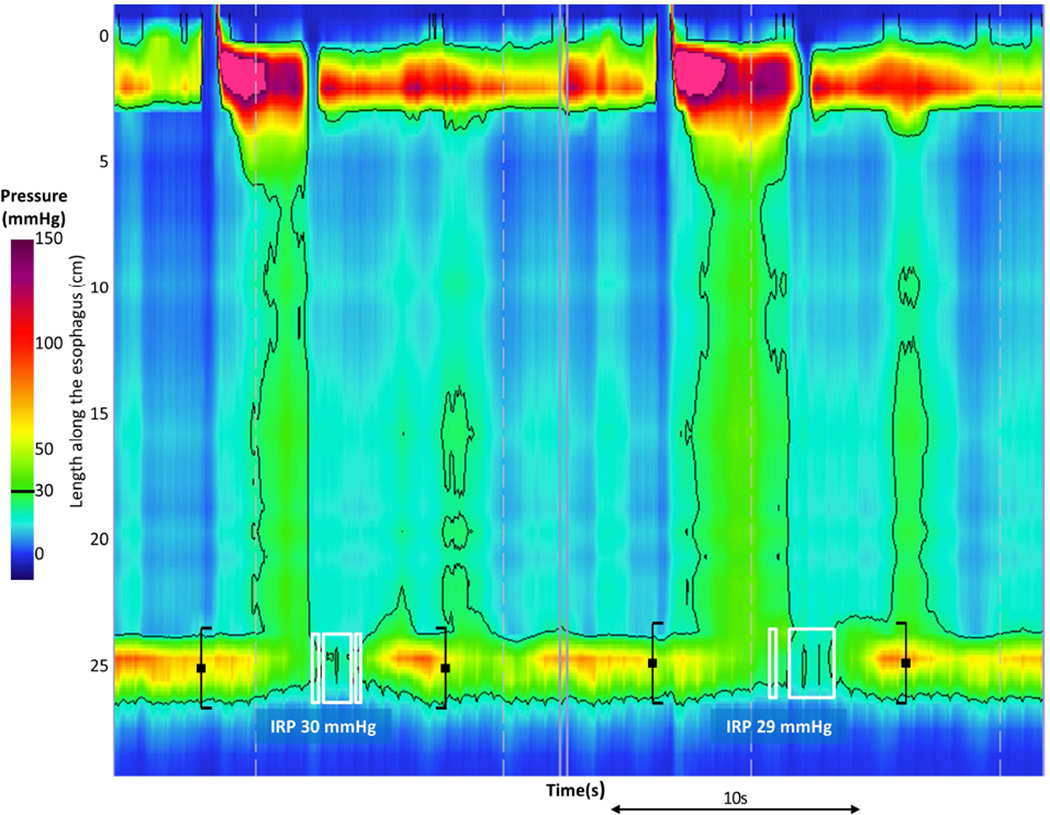
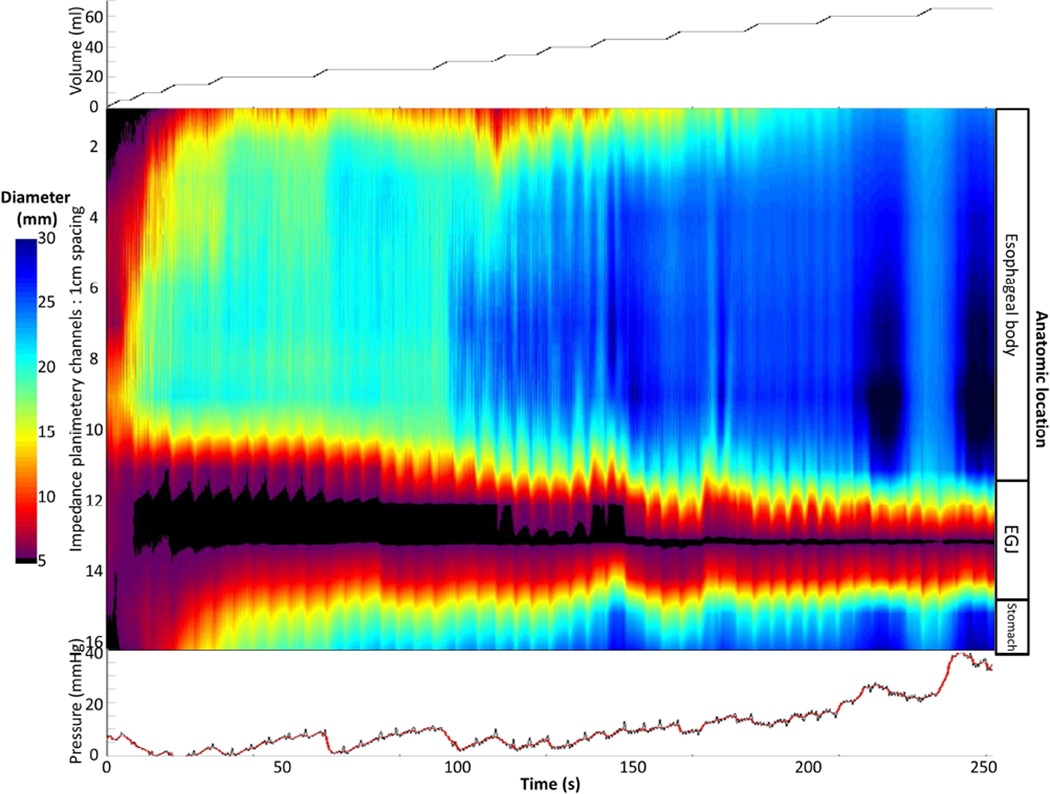
Methods: Fifty-one treatment-naive patients with achalasia, defined and subclassified by high-resolution esophageal pressure topography, and 10 asymptomatic individuals (controls) were evaluated with the FLIP during endoscopy. During stepwise distension, simultaneous intrabag pressures and 16 channels of cross-sectional areas were measured; data were exported to software that generated FLIP topography plots. Esophageal contractility was identified by noting periods of reduced luminal diameter. Esophageal contractions were characterized further by propagation direction, repetitiveness, and based on whether they were occluding or nonoccluding.
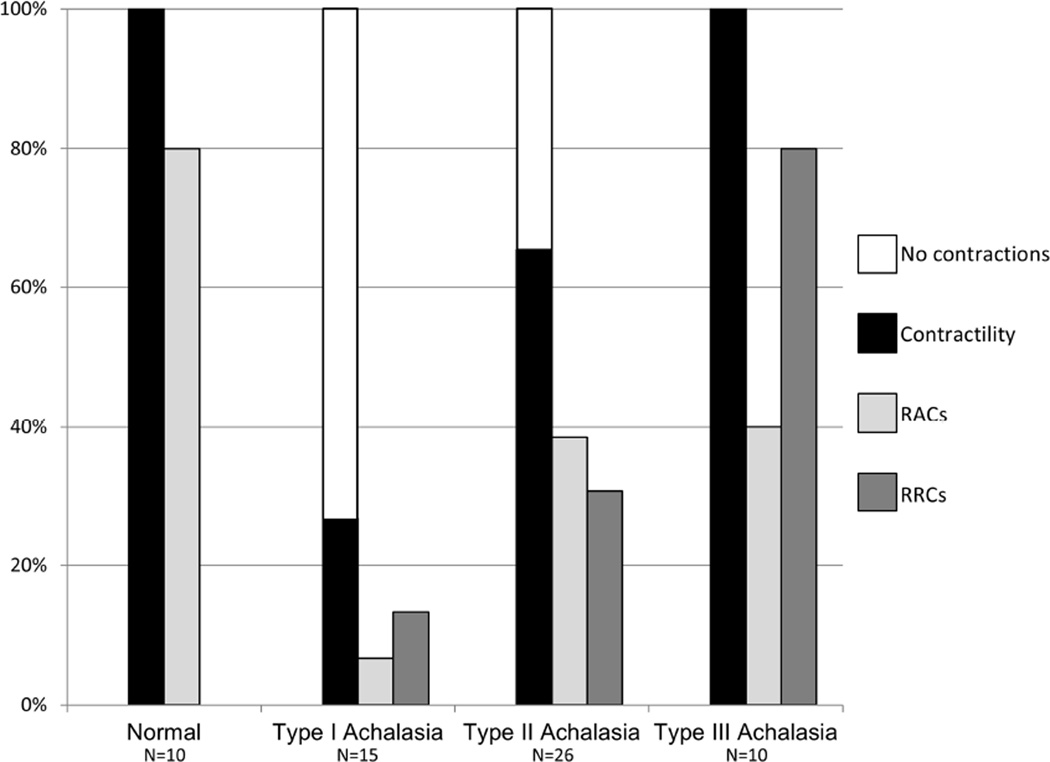
Results: Esophageal contractility was detected in all 10 controls: 8 of 10 had repetitive antegrade contractions and 9 of 10 had occluding contractions. Contractility was detected in 27% (4 of 15) of patients with type I achalasia and in 65% (18 of 26, including 9 with occluding contractions) of patients with type II achalasia. Contractility was detected in all 10 patients with type III achalasia; 8 of these patients had a pattern of contractility that was not observed in controls (repetitive retrograde contractions).
Conclusions: Esophageal contractility not observed with manometry can be detected in patients with achalasia using FLIP topography. The presence and patterns of contractility detected with FLIP topography may represent variations in pathophysiology, such as mechanisms of panesophageal pressurization in patients with type II achalasia. These findings could have implications for additional subclassification to supplement prediction of the achalasia disease course.
Keywords: EndoFLIP; Esophagus; Motility; Peristalsis.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of achalasia. The American journal of gastroenterology. 2013;108(8):1238–1249. quiz 50. - PubMed
-
- Salvador R, Costantini M, Zaninotto G, et al. The preoperative manometric pattern predicts the outcome of surgical treatment for esophageal achalasia. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2010;14(11):1635–1645. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
