

Using Modified RECIST and Alpha-Fetoprotein Levels to Assess Treatment Benefit in Hepatocellular Carcinoma
- PMID: 26280005
- PMCID: PMC4531422
- DOI: 10.1159/000343872
Using Modified RECIST and Alpha-Fetoprotein Levels to Assess Treatment Benefit in Hepatocellular Carcinoma
Abstract
Background and aims: Assessing treatment responses in hepatocellular carcinoma (HCC) is challenging, and alternative radiologic methods of measuring treatment response are required. Modified Response Evaluation Criteria in Solid Tumors (mRECIST) for HCC and alpha-fetoprotein (AFP) levels were assessed in a post hoc analysis of a phase II study of brivanib, a selective dual inhibitor of fibroblast growth factor and vascular endothelial growth factor signaling.
Methods: HCC patients were treated with first-line (cohort A; n = 55) or second-line (cohort B; n = 46) brivanib alaninate 800 mg once daily. Outcomes were compared between World Health Organization (WHO) criteria and (retrospectively by) mRECIST by independent review. The relationship between on-study AFP changes and outcome was analyzed in patients with elevated AFP at baseline.
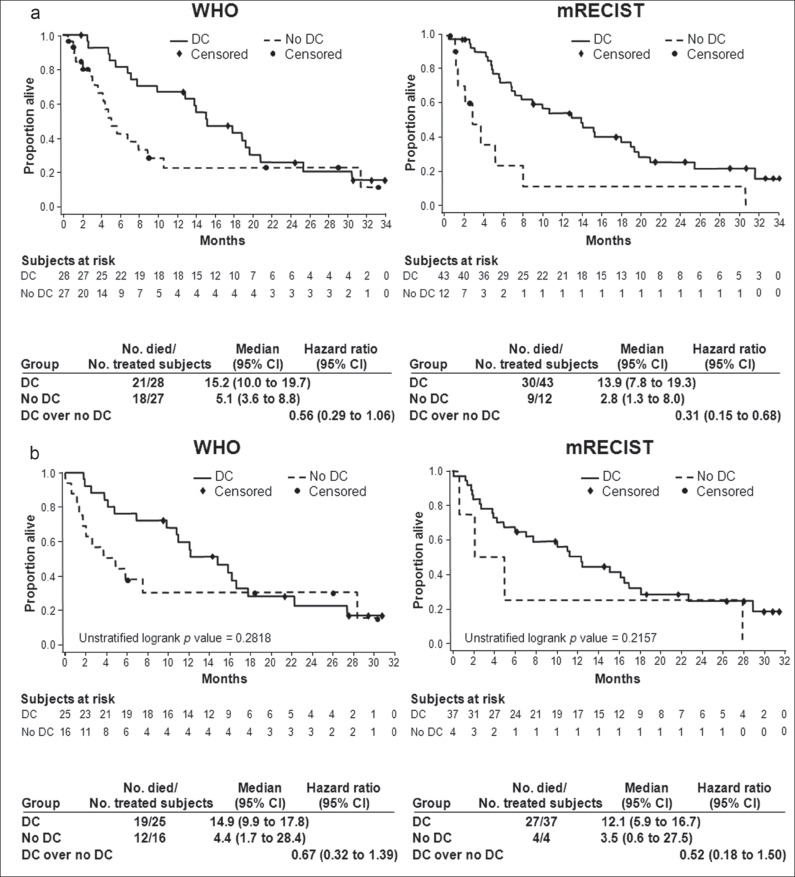
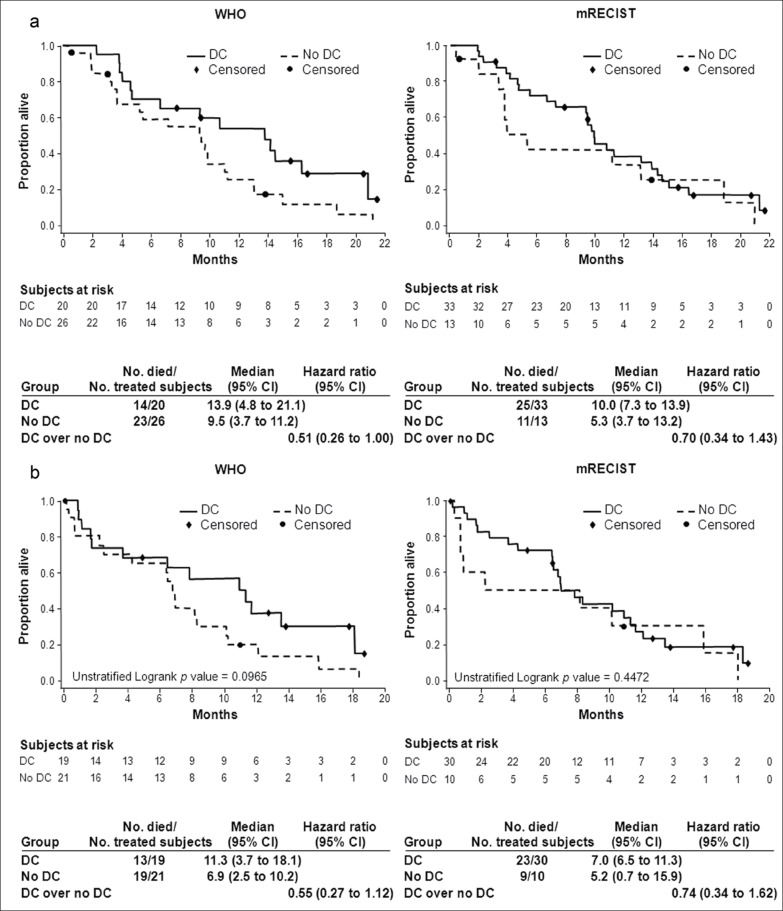
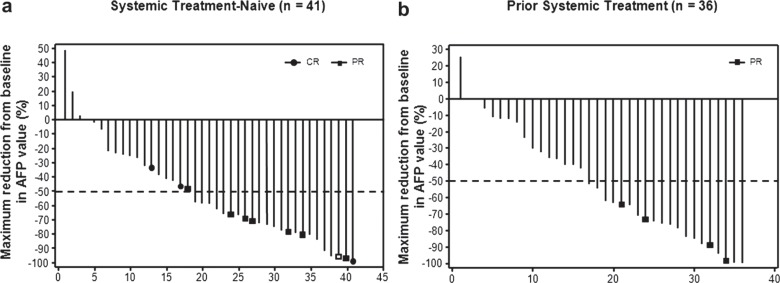
Results: Response rates were higher with mRECIST versus WHO criteria in cohorts A (25.5% vs. 7.3%) and B (10.9% vs. 4.3%). Progressive disease (PD) as assessed by mRECIST was associated with a very short median overall survival (OS; cohort A, 2.8 months; cohort B, 5.3 months); PD as assessed by WHO criteria reflected a mixed population of patients with better outcomes. mRECIST responders tended to have a>50% AFP decrease during therapy. In cohorts A and B pooled, an early AFP response (>20%or >50% decline from baseline within the first 4 weeks) was not associated with longer median OS.
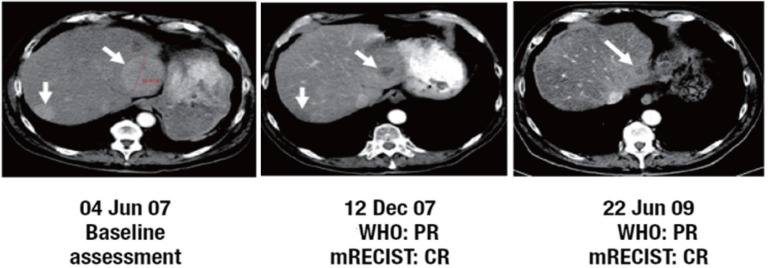
Conclusions: Tumor response as assessed by mRECIST differed from that by WHO criteria, with mRECIST possibly identifying true nonresponders with a poor prognosis. Many patients had AFP decreases correlating with tumor shrinkage, yet an association with long-term benefit was unclear. mRECIST and on-treatment AFP levels are being explored further with brivanib in HCC.
Keywords: Alpha-fetoprotein; Brivanib; Hepatocellular carcinoma; WHO criteria; mRECIST.
Figures
References
-
- Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, Bolondi L, Greten TF, Galle PR, Seitz JF, Borbath I, Hä ussinger D, Giannaris T, Shan M, Moscovici M, Voliotis D, Bruix J, SHARP Investigators Study Group Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378–390. - PubMed
-
- James K, Eisenhauer E, Christian M, Terenziani M, Vena D, Muldal A, Therasse P. Measuring response in solid tumors: unidimensional versus bidimensional measurement. J Natl Cancer Inst. 1999;91:523–528. - PubMed
-
- Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30:52–60. - PubMed
-
- Forner A, Ayuso C, Varela M, Rimola J, Hessheimer AJ, de Lope CR, Reig M, Bianchi L, Llovet JM, Bruix J. Evaluation of tumor response after locoregional therapies in hepatocellular carcinoma: are response evaluation criteria in solid tumors reliable? Cancer. 2009;115:616–623. - PubMed
-
- Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, Zhu AX, Sherman M, Schwartz M, Lotze M, Talwalkar J, Gores GJ, Panel of Experts in HCC-Design Clinical Trials Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst. 2008;100:698–711. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
