

JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan
- PMID: 26280007
- PMCID: PMC4531423
- DOI: 10.1159/000343875
JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan
Abstract
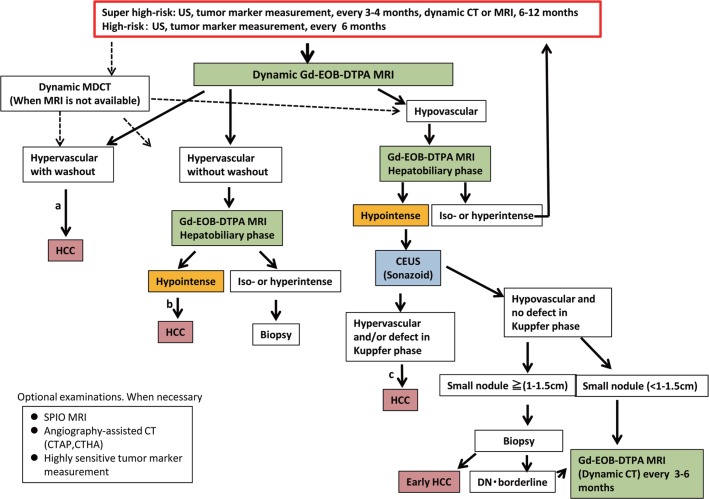
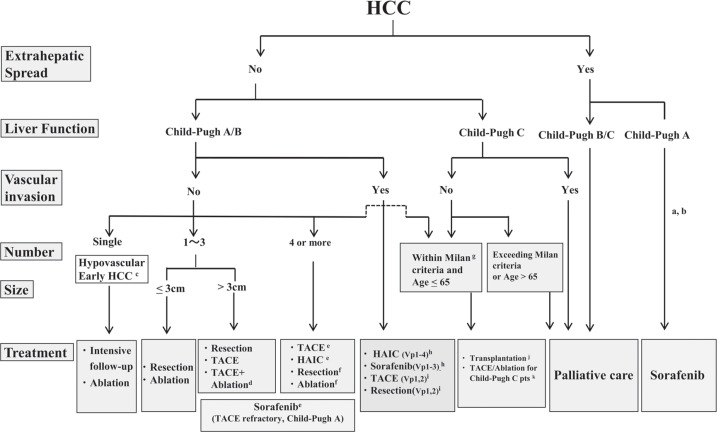
The Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma proposed by the Japan Society of Hepatology was updated in June 2014 at a consensus meeting of the Liver Cancer Study Group of Japan. Three important items have been updated: the surveillance and diagnostic algorithm, the treatment algorithm, and the definition of transarterial chemoembolization (TACE) failure/refractoriness. The most important update to the diagnostic algorithm is the inclusion of gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging as a first line surveillance/diagnostic tool. Another significant update concerns removal of the term "lipiodol" from the definition of TACE failure/refractoriness.
Keywords: Clinical practice guidelines; Definition of transarterial chemoembolization failure; Hepatocellular carcinoma; Japan Society of Hepatology; Liver Cancer Study Group of Japan.
Figures
References
-
- Kudo M, Izumi N, Kokudo N, Matsui O, Sakamoto M, Nakashima O, Kojiro M, Makuuchi M, HCC Expert Panel of Japan Society of Hepatology Management of hepatocellular carcinoma in Japan: Consensus-Based Clinical Practice Guidelines proposed by the Japan Society of Hepatology (JSH) 2010 updated version. Dig Dis. 2011;29:339–364. - PubMed
-
- Kudo M, Matsui O, Sakamoto M, Kitao A, Kim T, Ariizumi S, Ichikawa T, Kobayashi S, Imai Y, Izumi N, Fujinaga Y, Arii S. Role of gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid-enhanced magnetic resonance imaging in the management of hepatocellular carcinoma: consensus at the Symposium of the 48th Annual Meeting of the Liver Cancer Study Group of Japan. Oncology. 2013;84(Suppl 1):21–27. - PubMed
-
- Fujita N, Nishie A, Kubo Y, Asayama Y, Ushijima Y, Takayama Y, Moirta K, Shirabe K, Aishima S, Honda H. Hepatocellular carcinoma: clinical significance of signal heterogeneity in the hepatobiliary phase of gadoxetic acid-enhanced MR imaging. Eur Radiol 2014, Epub ahead of print. - PubMed
-
- Junqiang L, Yinzhong W, Li Z, Shunlin G, Xiaohui W, Yanan Z, Kehu Y. Gadoxetic acid disodium (Gd-EOBDTPA)-enhanced magnetic resonance imaging for the detection of hepatocellular carcinoma: a meta-analysis. J Magn Reson Imaging. 2014;39:1079–1087. - PubMed
-
- Faletti R, Cassinis MC, Fonio P, Bergamasco L, Pavan LJ, Rapellino A, David E, Gandini G. Multiparametric Gd-EOB-DTPA magnetic resonance in diagnosis of HCC: dynamic study, hepatobiliary phase, and diffusion-weighted imaging compared to histology after orthotopic liver transplantation. Abdom Imaging 2014, Epub ahead of print. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
