

Effect of Low-Density Lipoprotein Cholesterol Lowering by Ezetimibe/Simvastatin on Outcome Incidence: Overview, Meta-Analyses, and Meta-Regression Analyses of Randomized Trials
- PMID: 26282344
- PMCID: PMC6490854
- DOI: 10.1002/clc.22441
Effect of Low-Density Lipoprotein Cholesterol Lowering by Ezetimibe/Simvastatin on Outcome Incidence: Overview, Meta-Analyses, and Meta-Regression Analyses of Randomized Trials
Abstract
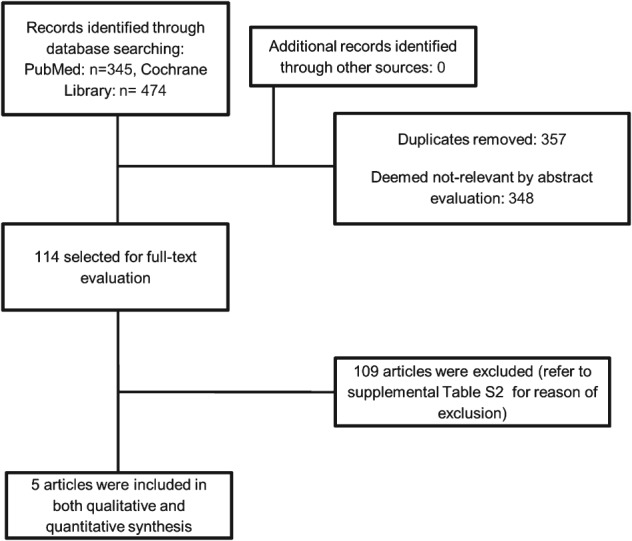
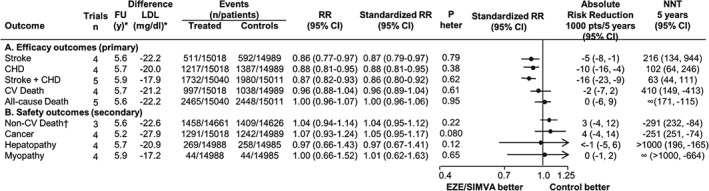
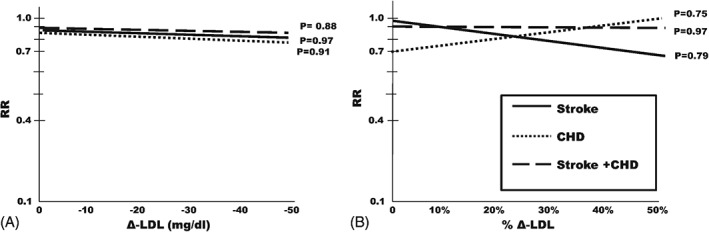
This analysis investigated the extent of different outcome reductions from low-density lipoprotein cholesterol (LDL-C) lowering following ezetimibe/simvastatin treatment and the proportionality of outcome to LDL-C reductions. The authors searched PubMed between 1997 and mid-June 2015 (any language) and the Cochrane Library to identify all randomized controlled trials comparing ezetimibe/simvastatin with placebo or less intensive LDL-C lowering. Risk ratios (RR) and 95% confidence intervals (CIs), standardized to 20 mg/dL LDL-C reduction, were calculated for 5 primary outcomes (fatal and nonfatal) and 4 secondary outcomes (non-cardiovascular [CV] death, cancer, myopathy, and hepatopathy). Five ezetimibe/simvastatin RCTs (30 051 individuals) were eligible, 2 comparing ezetimibe/simvastatin vs placebo and 3 vs less intensive treatment. Outcomes reduced almost to the same extent were stroke (RR: -13%, 95% CI: -21% to -3%), coronary heart disease (CHD; RR: -12%, 95% CI: -19% to -5%), and composite of stroke and CHD (RR: -14%, 95% CI: -20% to -8%). Absolute risk reductions: 5 strokes, 10 CHD events, and 16 stroke and CHD events prevented for every 1000 patients treated for 5 years. Residual risk was almost 7× higher than absolute risk reduction for all the above outcomes. All death outcomes were not reduced, and secondary outcomes did not differ between groups. Logarithmic risk ratios were not associated with LDL-C lowering. Our meta-analysis provides evidence that, in patients with different CV disease burden, major CV events are safely reduced by LDL-C lowering with ezetimibe/simvastatin, while raising the hypothesis that the extent of LDL-C lowering might not be accompanied by incremental clinical-event reduction.
© 2015 Wiley Periodicals, Inc.
Figures
References
-
- Di Napoli P, Taccardi AA, Oliver M, et al. Statins and stroke: evidence for cholesterol‐independent effects. Eur Heart J. 2002;23:1908–1921. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines [published correction appears in J Am Coll Cardiol. 2014;63(25 part B):3024–3025]. J Am Coll Cardiol. 2014;63(25 part B):2889–2934. - PubMed
-
- Morrone D, Weintraub WS, Toth PP, et al. Lipid‐altering efficacy of ezetimibe plus statin and statin monotherapy and identification of factors associated with treatment response: a pooled analysis of over 21 000 subjects from 27 clinical trials. Atherosclerosis. 2012;223:251–261. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
