

A prospective study comparing radiographer- and clinician-based localization for patients with metastatic spinal cord compression (MSCC) to assess the feasibility of a radiographer-led service
- PMID: 26283103
- PMCID: PMC4743470
- DOI: 10.1259/bjr.20150586
A prospective study comparing radiographer- and clinician-based localization for patients with metastatic spinal cord compression (MSCC) to assess the feasibility of a radiographer-led service
Abstract
Objective: To investigate whether there was parity between treatment fields localized by radiographers and clinicians, by comparing geographical variations and hence determining the feasibility of a radiographer-led service.
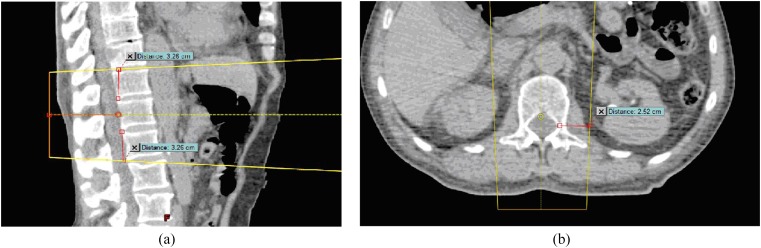
Methods: 23 patients with metastatic spinal cord compression (MSCC) were prospectively sampled. Four radiographers not involved in the original planning performed localization on each patient. The 92 localizations that they determined were compared with the clinician-approved fields. Agreement was defined as ≤0.5 cm between field length, width and three isocentre co-ordinates. To be feasible, agreement was required in a minimum of 97% of the cases. The potential time saved with a radiographer-led approach was also recorded.
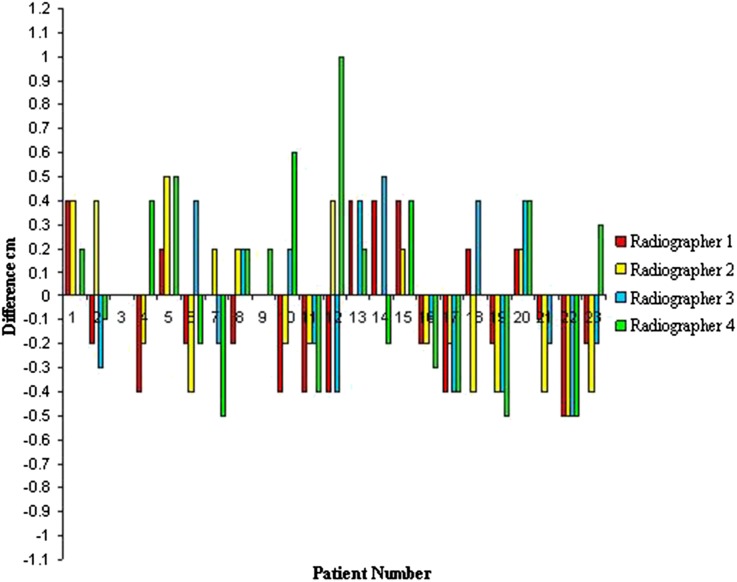
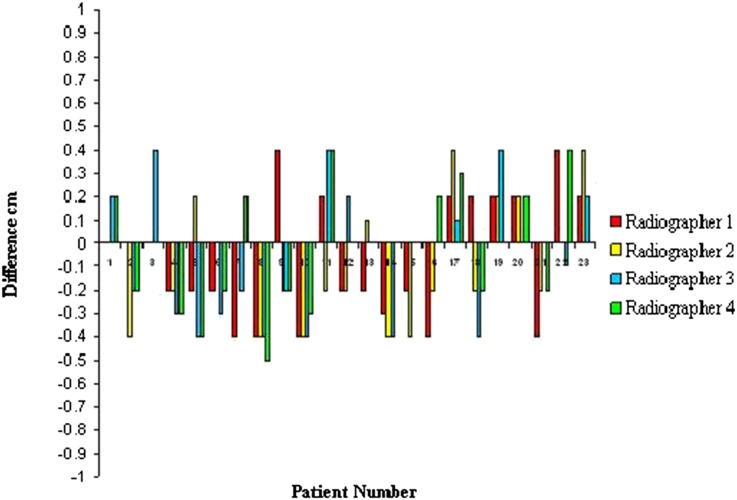
Results: Agreement between clinicians and radiographers was 97.8%. For all field parameters, the average differences were <0.3 cm and were significantly different from the 0.5-cm median (p < 0.0001) that would establish no agreement using Wilcoxon signed-rank test. The average (range) delay awaiting clinician approval was 54 min (4-141 min).
Conclusion: Strong agreement between radiographer and clinician localizations was established. It was also highlighted that time could be saved in the patient's pathway by removing the need to wait for clinician approval. We believe this supports a radiographer-led service.
Advances in knowledge: This article is novel, as it is the first known comparison between clinicians and radiographers in the localization of MSCC radiotherapy. These data show the feasibility of introducing radiographer-led practice and a methodology that could be potentially transferred to investigate the localization parity for other treatment sites.
Figures


References
-
- Hoskin P, Grover A, Bhana R. Metastatic spinal cord compression: radiotherapy outcome and dose fractionation. Radiother Oncol 2003; 68: 175–80. - PubMed
-
- Guideline NICE. Metastatic spinal cord compression: diagnosis and management of patients at risk of or with metastatic spinal cord compression. London, UK: National Institute for Health and Clinical Excellence National Collaborating Centre Cancer; 2008. - PubMed
-
- Halweg-Larsen S, Sørensen PS, Kreiner S. Prognostic factors in metastatic spinal cord compression: a prospective study using multivariate analysis of variables influencing survival and gait function in 153 patients. Int J Radiat Oncol Biol Phys 2000; 46: 1163–9. - PubMed
-
- Cancer Research UK. UK cancer incidence statistics. London, UK: Cancer Research UK; 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
