

Utility of magnetic resonance imaging in the differential diagnosis of tubercular and pyogenic spondylodiscitis
- PMID: 26283836
- PMCID: PMC4518416
- DOI: 10.4103/0976-9668.160016
Utility of magnetic resonance imaging in the differential diagnosis of tubercular and pyogenic spondylodiscitis
Abstract
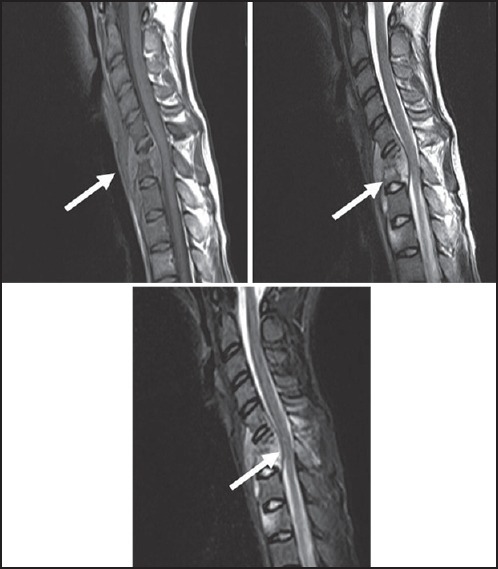
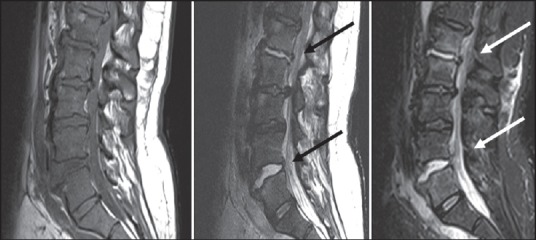
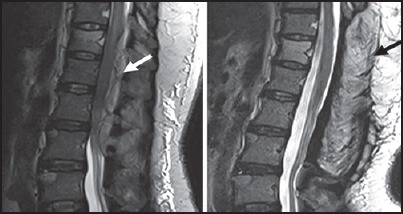
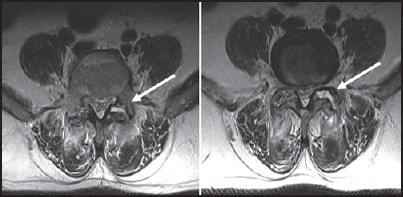
Aim: We evaluated the potential of magnetic resonance imaging (MRI) in the diagnosis of spinal infections and specifically its accuracy in differentiating tubercular and pyogenic spondylodiscitis.
Materials and methods: Totally, 50 patients referred for MRI scans with the clinical diagnosis of spinal infections were included in our study. The patients were classified as tubercular (TS), pyogenic (PS), and indeterminate spondylodiscitis on the basis of imaging findings and were correlated with the final diagnosis made by histopathology/cytology/culture/biochemistry or with successful therapeutic outcome. Imaging findings were subsequently analyzed for differentiating tubercular and pyogenic spondylodiscitis using the Chi-square test.
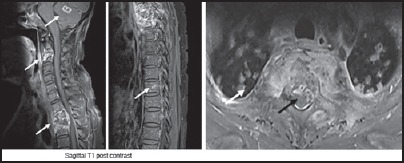
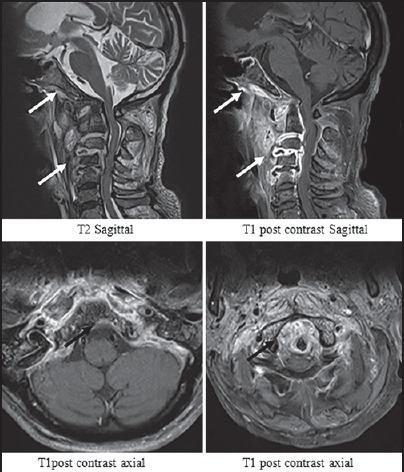
Results: The most common pattern of spinal infection was spondylodiscitis (78% incidence rate) with epidural extension (86%) and cord compression (64%) being most common complications observed. Imaging (postcontrast study) and final diagnosis correlated in 93.7% tubercular (sensitivity of 75% and specificity of 90%) and 75% pyogenic (sensitivity of 90% and specificity of 83.3%) spondylodiscitis. The patients with tubercular spondylitis had a significantly (P < 0.05) higher incidence of following MRI findings: A well-defined paraspinal abnormal signal (80% in TS vs. 40% in PS), a thin and smooth abscess wall (84.2% in TS vs. 10% in PS), presence of intraosseous abscess (35% in TS vs. 0% in PS), focal and heterogenous enhancement of the vertebral body (75% in TS vs. 20% in PS), vertebral destruction more than or equal to grade 3 (71.8% in TS vs. 0% in PS), loss of cortical definition (75% in TS vs. 20% in PS), and spinal deformity (50% in TS vs. 5% in PS).
Conclusion: Contrast-enhanced images improve the sensitivity and specificity of detection and differentiation of tubercular and PS.
Keywords: Cortical destruction; magnetic resonance imaging; spondylitis.
Conflict of interest statement
Figures


References
-
- Jung NY, Jee WH, Ha KY, Park CK, Byun JY. Discrimination of tuberculous spondylitis from pyogenic spondylitis on MRI. AJR Am J Roentgenol. 2004;182:1405–10. - PubMed
-
- Stäbler A, Reiser MF. Imaging of spinal infection. Radiol Clin North Am. 2001;39:115–35. - PubMed
-
- Varma R, Lander P, Assaf A. Imaging of pyogenic infectious spondylodiskitis. Radiol Clin North Am. 2001;39:203–13. - PubMed
-
- Tins BJ, Cassar-Pullicino VN. MR imaging of spinal infection. Semin Musculoskelet Radiol. 2004;8:215–29. - PubMed
-
- Moore SL, Rafii M. Imaging of musculoskeletal and spinal tuberculosis. Radiol Clin North Am. 2001;39:329–42. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources