

Septic Shock: Advances in Diagnosis and Treatment
- PMID: 26284722
- PMCID: PMC4646706
- DOI: 10.1001/jama.2015.7885
Septic Shock: Advances in Diagnosis and Treatment
Erratum in
-
Incorrect Title for Table.JAMA. 2015 Oct 6;314(13):1404. doi: 10.1001/jama.2015.11164. JAMA. 2015. PMID: 26441192 No abstract available.
Abstract
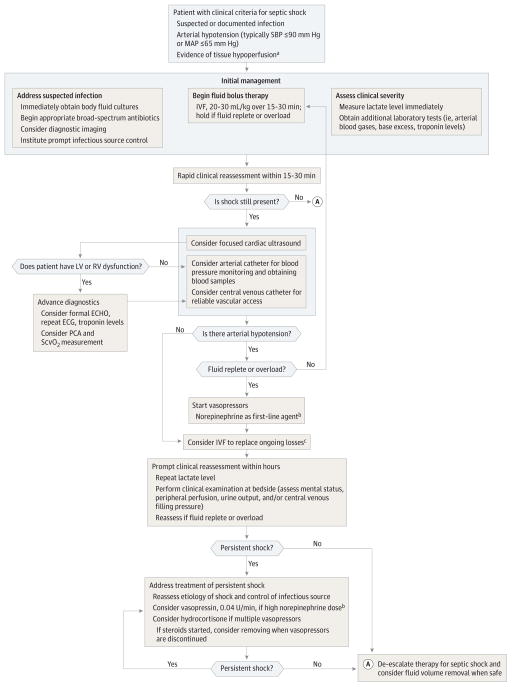
Importance: Septic shock is a clinical emergency that occurs in more than 230,000 US patients each year. OBSERVATIONS AND ADVANCES: In the setting of suspected or documented infection, septic shock is typically defined in a clinical setting by low systolic (≤90 mm Hg) or mean arterial blood pressure (≤65 mm Hg) accompanied by signs of hypoperfusion (eg, oliguria, hyperlactemia, poor peripheral perfusion, or altered mental status). Focused ultrasonography is recommended for the prompt recognition of complicating physiology (eg, hypovolemia or cardiogenic shock), while invasive hemodynamic monitoring is recommended only for select patients. In septic shock, 3 randomized clinical trials demonstrate that protocolized care offers little advantage compared with management without a protocol. Hydroxyethyl starch is no longer recommended, and debate continues about the role of various crystalloid solutions and albumin.
Conclusions and relevance: The prompt diagnosis of septic shock begins with obtainment of medical history and performance of a physical examination for signs and symptoms of infection and may require focused ultrasonography to recognize more complex physiologic manifestations of shock. Clinicians should understand the importance of prompt administration of intravenous fluids and vasoactive medications aimed at restoring adequate circulation, and the limitations of protocol-based therapy, as guided by recent evidence.
Conflict of interest statement
Figures
Comment in
-
Bedside Ultrasonography for Diagnosis of Septic Shock.JAMA. 2016 Jan 5;315(1):89. doi: 10.1001/jama.2015.15061. JAMA. 2016. PMID: 26746466 No abstract available.
-
Bedside Ultrasonography for Diagnosis of Septic Shock--Reply.JAMA. 2016 Jan 5;315(1):89-90. doi: 10.1001/jama.2015.15073. JAMA. 2016. PMID: 26746467 No abstract available.
References
-
- Walley KR, Wood LDH. Shock. In: Hall J, Wood LDH, editors. Principles of Critical Care. New York, NY: McGraw Hill Co; 1998. pp. 277–301.
-
- Millham FH. A brief history of shock. Surgery. 2010;148(5):1026–1037. - PubMed
-
- Manji RA, Wood KE, Kumar A. The history and evolution of circulatory shock. Crit Care Clin. 2009;25(1):1–29. - PubMed
-
- Weil MH, Shubin H. Proposed reclassification of shock states with special reference to distributive defects. Adv Exp Med Biol. 1971;23(0):13–23. - PubMed
-
- Parker MM, Shelhamer JH, Bacharach SL, et al. Profound but reversible myocardial depression in patients with septic shock. Ann Intern Med. 1984;100(4):483–490. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
