

The Physiologic Impact of Unilateral Recurrent Laryngeal Nerve (RLN) Lesion on Infant Oropharyngeal and Esophageal Performance
- PMID: 26285799
- PMCID: PMC4639401
- DOI: 10.1007/s00455-015-9648-8
The Physiologic Impact of Unilateral Recurrent Laryngeal Nerve (RLN) Lesion on Infant Oropharyngeal and Esophageal Performance
Abstract
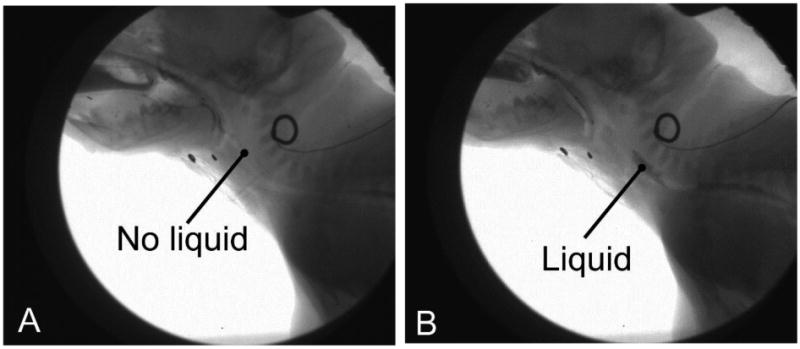
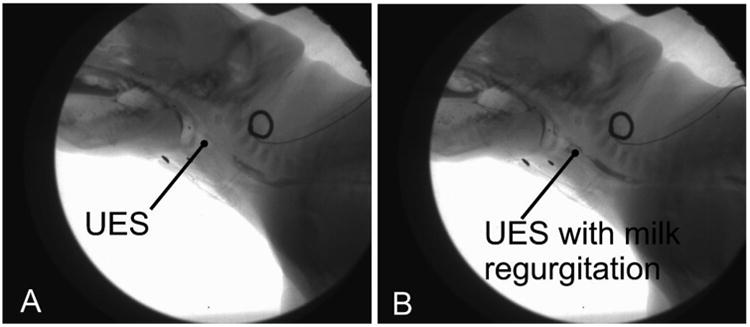
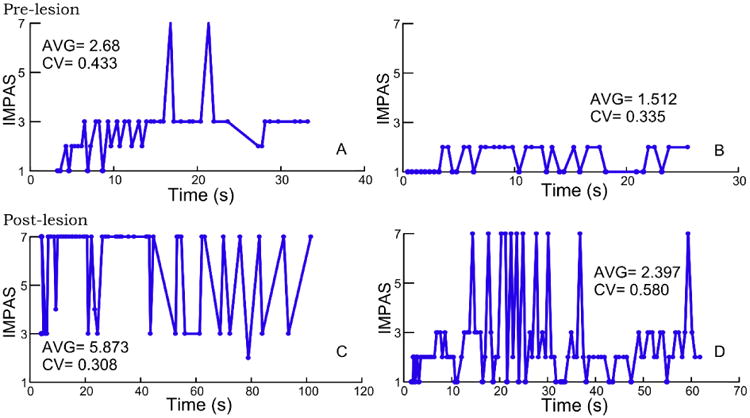
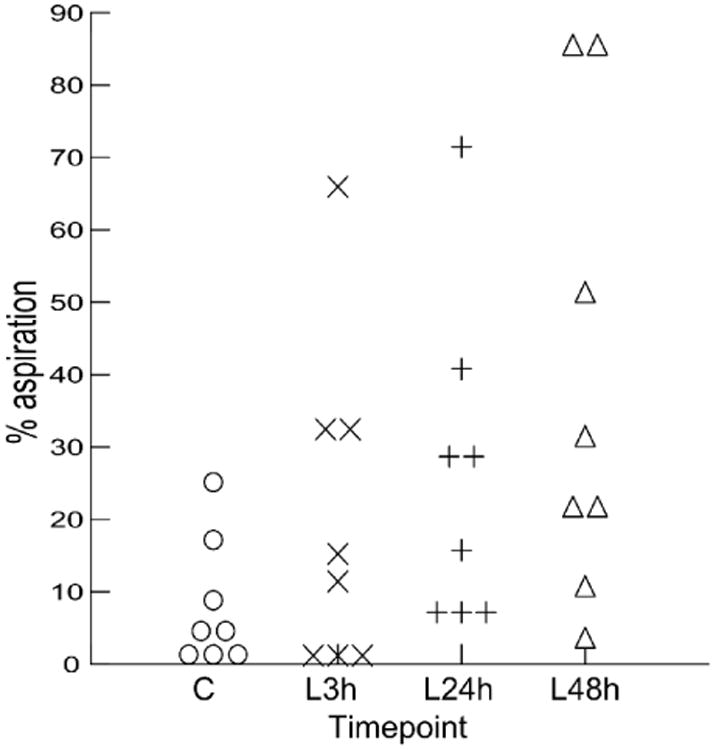
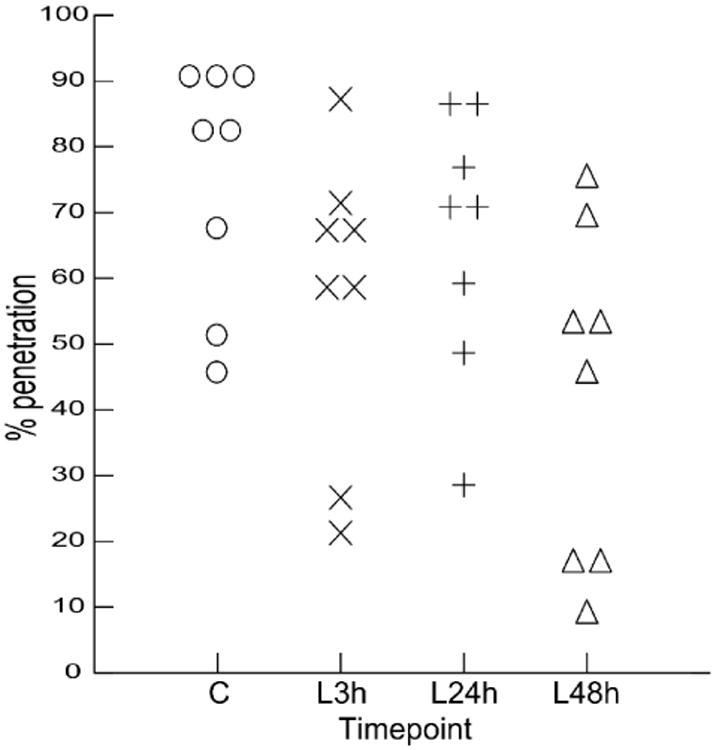
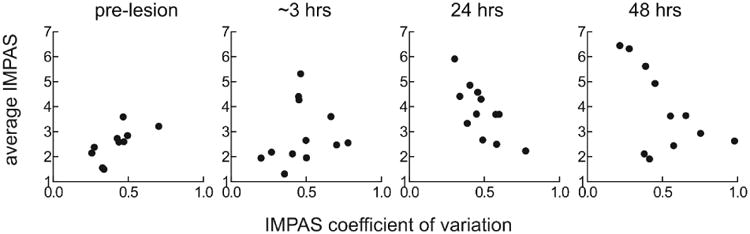
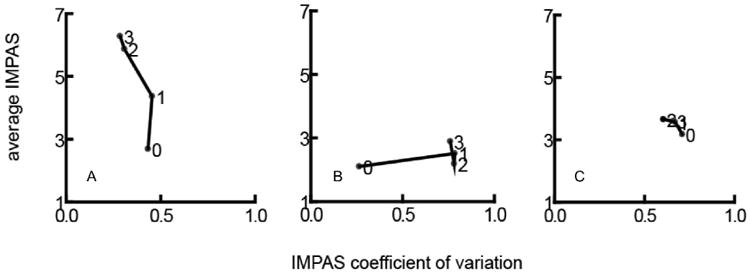
Recurrent laryngeal nerve (RLN) injury in neonates, a complication of patent ductus arteriosus corrective surgery, leads to aspiration and swallowing complications. Severity of symptoms and prognosis for recovery are variable. We transected the RLN unilaterally in an infant mammalian animal model to characterize the degree and variability of dysphagia in a controlled experimental setting. We tested the hypotheses that (1) both airway protection and esophageal function would be compromised by lesion, (2) given our design, variability between multiple post-lesion trials would be minimal, and (3) variability among individuals would be minimal. Individuals' swallowing performance was assessed pre- and post-lesion using high speed VFSS. Aspiration was assessed using the Infant Mammalian Penetration-Aspiration Scale (IMPAS). Esophageal function was assessed using two measures devised for this study. Our results indicate that RLN lesion leads to increased frequency of aspiration, and increased esophageal dysfunction, with significant variation in these basic patterns at all levels. On average, aspiration worsened with time post-lesion. Within a single feeding sequence, the distribution of unsafe swallows varied. Individuals changed post-lesion either by increasing average IMPAS score, or by increasing variation in IMPAS score. Unilateral RLN transection resulted in dysphagia with both compromised airway protection and esophageal function. Despite consistent, experimentally controlled injury, significant variation in response to lesion remained. Aspiration following RLN lesion was due to more than unilateral vocal fold paralysis. We suggest that neurological variation underlies this pattern.
Keywords: Aspiration; Deglutition; Deglutition disorders; Esophagus; Infant; Recurrent laryngeal nerve.
Conflict of interest statement
Figures
References
-
- Pereira KD, Webb BD, Blakely ML, Cox CS, Jr, Lally KP. Sequelae of recurrent laryngeal nerve injury after patent ductus arteriosus ligation. International Journal of Pediatric Otorhinolaryngology. 2006;70:1609–12. - PubMed
-
- Nichols BG, Jabbour J, Hehir DA, Ghanayem NS, Beste D, Martin T, et al. Recovery of vocal fold immobility following isolated patent ductus arteriosus ligation. International Journal of Pediatric Otorhinolaryngology. 2014;78:1316–9. - PubMed
-
- De Gaudemar I, Roudaire M, François M, Narcy P. Outcome of laryngeal paralysis in neonates: a long term retrospective study of 113 cases. International Journal of Pediatric Otorhinolaryngology. 1996;34:101–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
