

Alterations of the Subgingival Microbiota in Pediatric Crohn's Disease Studied Longitudinally in Discovery and Validation Cohorts
- PMID: 26288001
- PMCID: PMC4950860
- DOI: 10.1097/MIB.0000000000000557
Alterations of the Subgingival Microbiota in Pediatric Crohn's Disease Studied Longitudinally in Discovery and Validation Cohorts
Abstract
Background: Oral manifestations are common in Crohn's disease (CD). Here we characterized the subgingival microbiota in pediatric patients with CD initiating therapy and after 8 weeks to identify microbial community features associated with CD and therapy.
Methods: Pediatric patients with CD were recruited from The Children's Hospital of Pennsylvania. Healthy control subjects were recruited from primary care or orthopedics clinic. Subgingival plaque samples were collected at initiation of therapy and after 8 weeks. Treatment exposures included 5-ASAs, immunomodulators, steroids, and infliximab. The microbiota was characterized by 16S rRNA gene sequencing. The study was repeated in separate discovery (35 CD, 43 healthy) and validation cohorts (43 CD, 31 healthy).
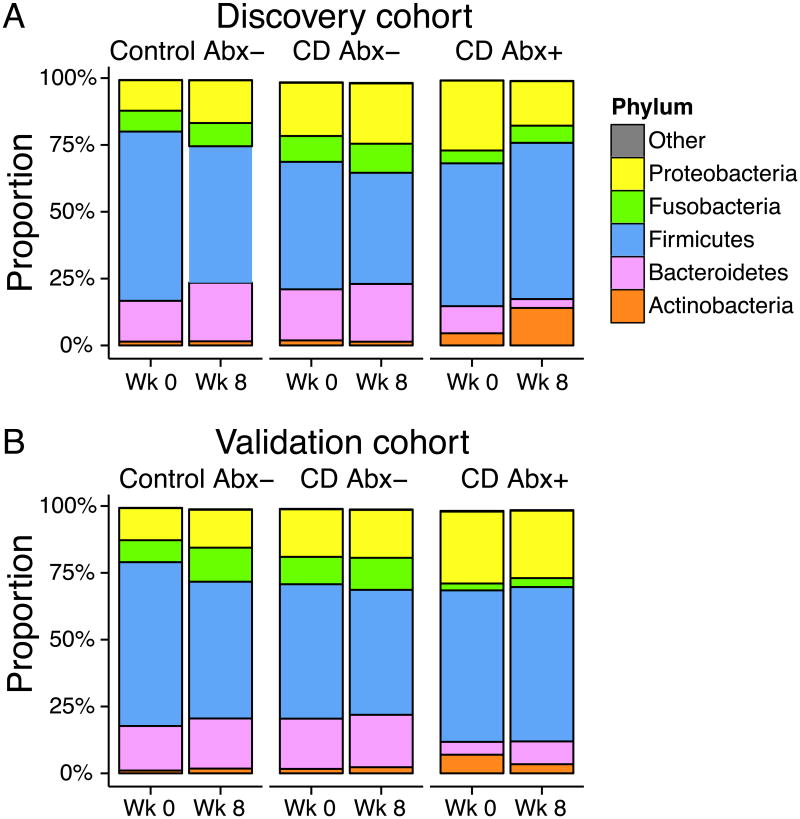
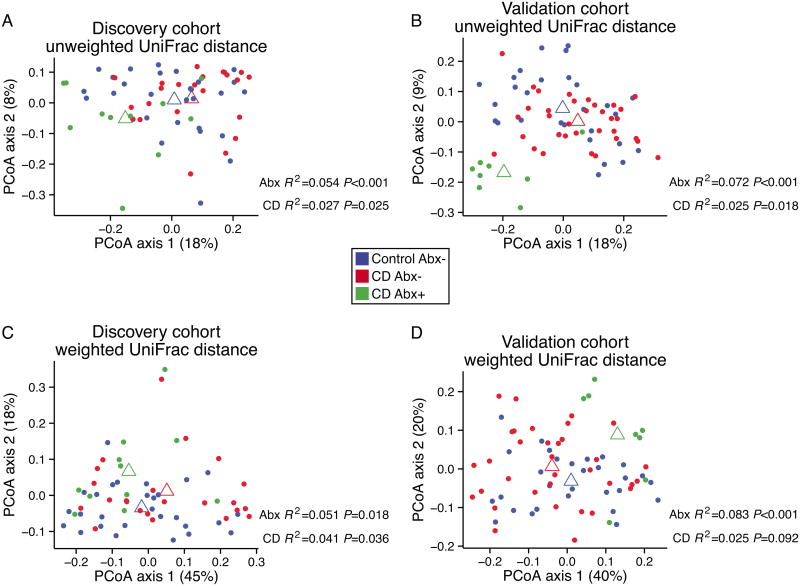
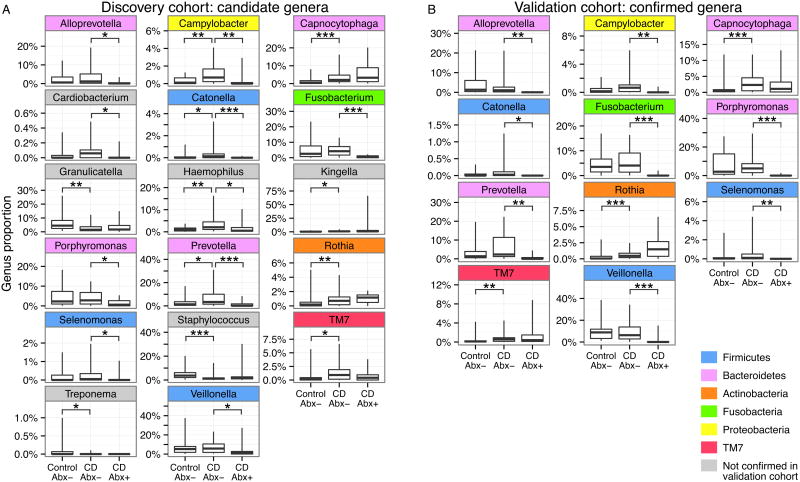
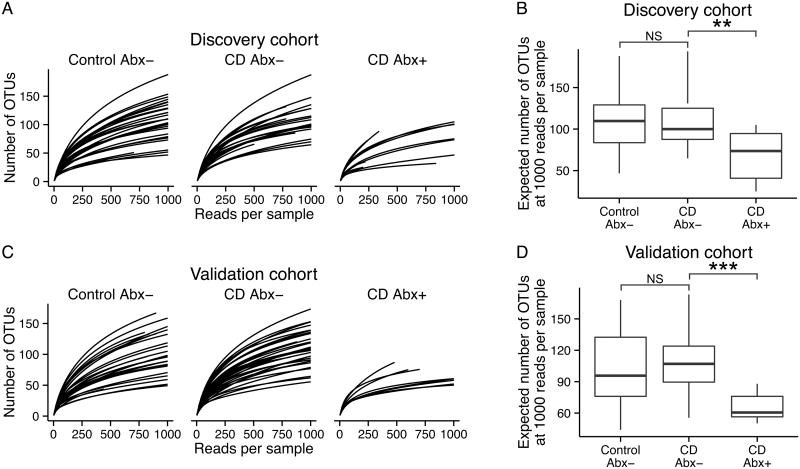
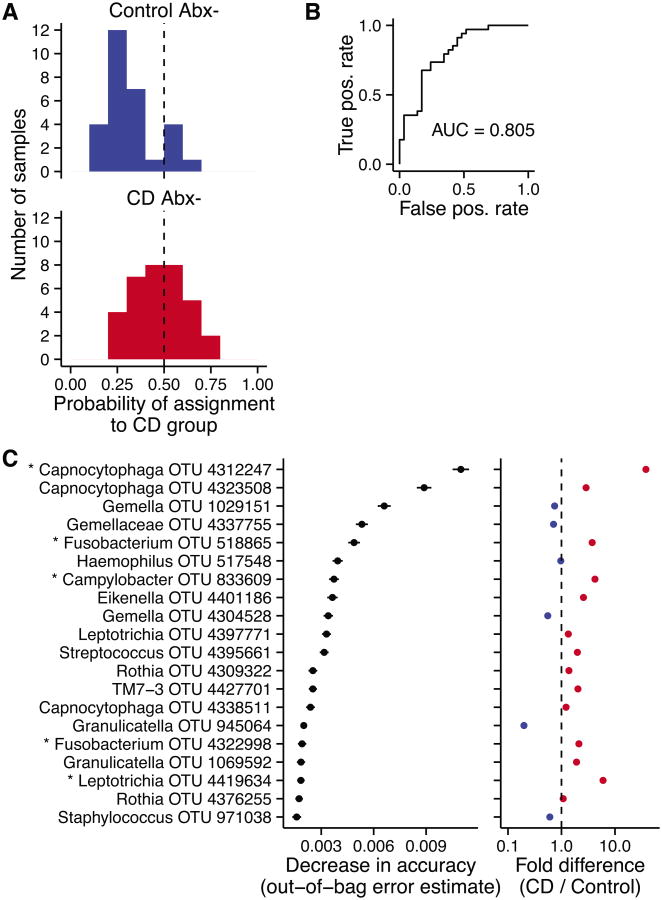
Results: Most subjects in both cohorts demonstrated clinical response after 8 weeks of therapy (discovery cohort 88%, validation cohort 79%). At week 0, both antibiotic exposure and disease state were associated with differences in bacterial community composition. Seventeen genera were identified in the discovery cohort as candidate biomarkers, of which 11 were confirmed in the validation cohort. Capnocytophaga, Rothia, and TM7 were more abundant in CD relative to healthy controls. Other bacteria were reduced in abundance with antibiotic exposure among CD subjects. CD-associated genera were not enriched compared with healthy controls after 8 weeks of therapy.
Conclusions: Subgingival microbial community structure differed with CD and antibiotic use. Results in the discovery cohort were replicated in a separate validation cohort. Several potentially pathogenic bacterial lineages were associated with CD but were not diminished in abundance by antibiotic treatment, suggesting targets for additional surveillance.
Conflict of interest statement
The authors have no potential conflicts to disclose.
Figures
Similar articles
-
Characteristics of Faecal Microbiota in Paediatric Crohn's Disease and Their Dynamic Changes During Infliximab Therapy.J Crohns Colitis. 2018 Feb 28;12(3):337-346. doi: 10.1093/ecco-jcc/jjx153. J Crohns Colitis. 2018. PMID: 29194468
-
Does the intestinal microbial community of Korean Crohn's disease patients differ from that of western patients?BMC Gastroenterol. 2016 Feb 29;16:28. doi: 10.1186/s12876-016-0437-0. BMC Gastroenterol. 2016. PMID: 26922889 Free PMC article.
-
Fecal Microbiota Alterations Associated With Clinical and Endoscopic Response to Infliximab Therapy in Crohn's Disease.Inflamm Bowel Dis. 2020 Oct 23;26(11):1636-1647. doi: 10.1093/ibd/izaa253. Inflamm Bowel Dis. 2020. PMID: 33026078
-
Natalizumab for induction of remission in Crohn's disease.Cochrane Database Syst Rev. 2018 Aug 1;8(8):CD006097. doi: 10.1002/14651858.CD006097.pub3. Cochrane Database Syst Rev. 2018. PMID: 30068022 Free PMC article.
-
Update on the management of Crohn's disease.Curr Gastroenterol Rep. 2011 Oct;13(5):465-74. doi: 10.1007/s11894-011-0220-x. Curr Gastroenterol Rep. 2011. PMID: 21792543 Review.
Cited by
-
Antibiotics in inflammatory bowel diseases: do we know what we're doing?Transl Pediatr. 2019 Jan;8(1):42-55. doi: 10.21037/tp.2018.11.02. Transl Pediatr. 2019. PMID: 30881898 Free PMC article. Review.
-
A pilot study of the use of the oral and faecal microbiota for the diagnosis of ulcerative colitis and Crohn's disease in a paediatric population.Front Pediatr. 2023 Nov 16;11:1220976. doi: 10.3389/fped.2023.1220976. eCollection 2023. Front Pediatr. 2023. PMID: 38034829 Free PMC article.
-
The role of oral bacteria in inflammatory bowel disease.Nat Rev Gastroenterol Hepatol. 2021 Oct;18(10):731-742. doi: 10.1038/s41575-021-00488-4. Epub 2021 Aug 16. Nat Rev Gastroenterol Hepatol. 2021. PMID: 34400822 Review.
-
Comparative study on the pathogenesis of Crohn's disease and ulcerative colitis.World J Gastroenterol. 2025 May 21;31(19):106406. doi: 10.3748/wjg.v31.i19.106406. World J Gastroenterol. 2025. PMID: 40497094 Free PMC article. Review.
-
Dysbiosis, inflammation, and response to treatment: a longitudinal study of pediatric subjects with newly diagnosed inflammatory bowel disease.Genome Med. 2016 Jul 13;8(1):75. doi: 10.1186/s13073-016-0331-y. Genome Med. 2016. PMID: 27412252 Free PMC article.
References
-
- Plauth M, Jenss H, Meyle J. Oral manifestations of Crohn's disease. An analysis of 79 cases. J Clin Gastroenterol. 1991;13:29–37. - PubMed
-
- Pittock S, Drumm B, Fleming P, et al. The oral cavity in Crohn's disease. J Pediatr. 2001;138:767–771. - PubMed
-
- Harty S, Fleming P, Rowland M, et al. A prospective study of the oral manifestations of Crohn's disease. Clin Gastroenterol Hepatol. 2005;3:886–891. - PubMed
-
- Hovav AH. Dendritic cells of the oral mucosa. Mucosal Immunol. 2014;7:27–37. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
