

Chest tuberculosis: Radiological review and imaging recommendations
- PMID: 26288514
- PMCID: PMC4531444
- DOI: 10.4103/0971-3026.161431
Chest tuberculosis: Radiological review and imaging recommendations
Abstract
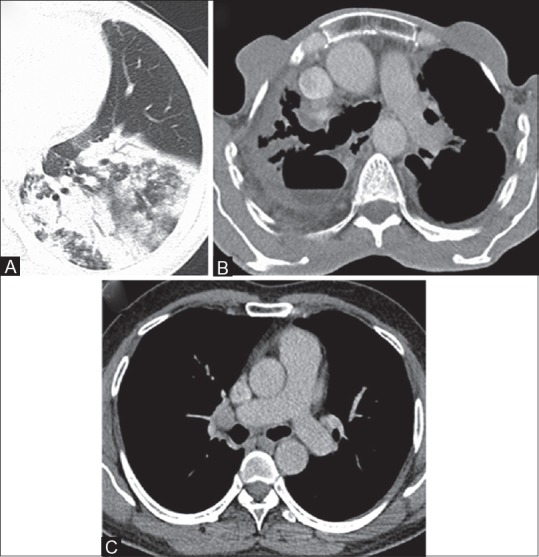
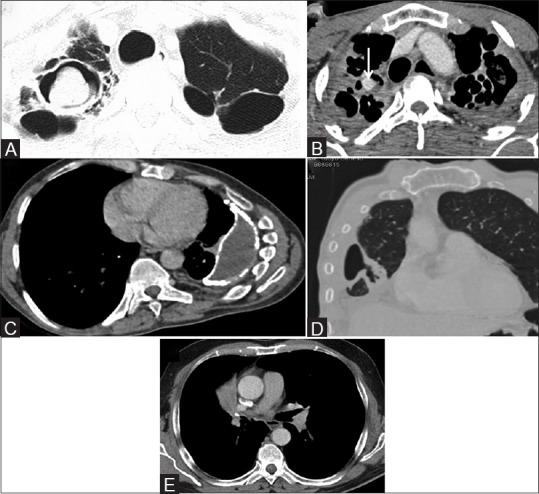
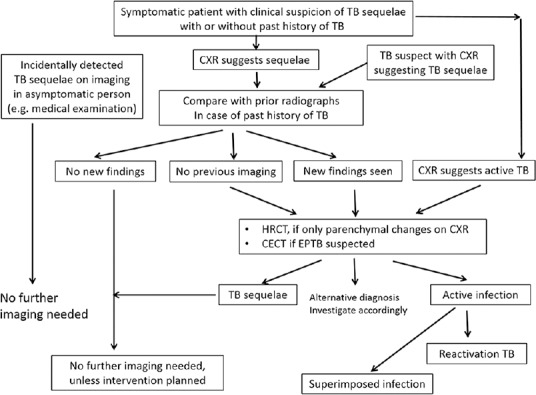
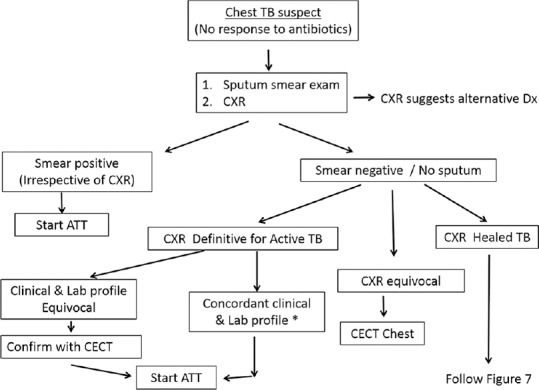
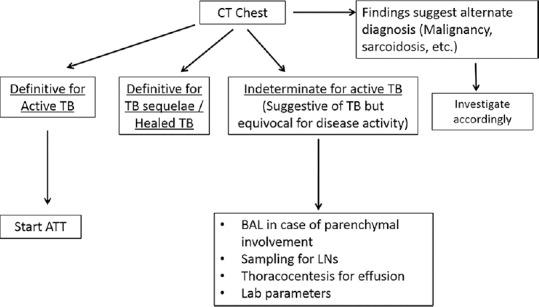
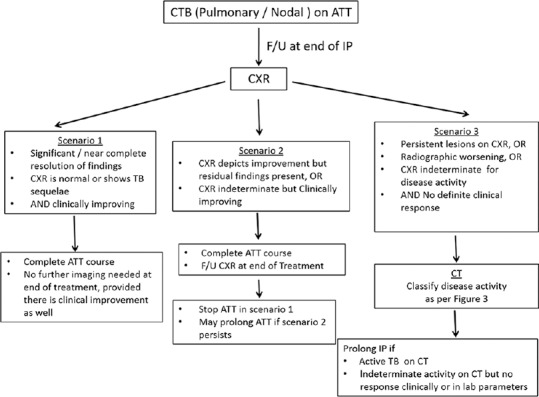
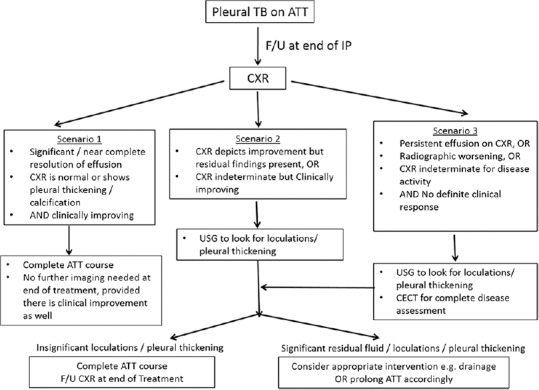
Chest tuberculosis (CTB) is a widespread problem, especially in our country where it is one of the leading causes of mortality. The article reviews the imaging findings in CTB on various modalities. We also attempt to categorize the findings into those definitive for active TB, indeterminate for disease activity, and those indicating healed TB. Though various radiological modalities are widely used in evaluation of such patients, no imaging guidelines exist for the use of these modalities in diagnosis and follow-up. Consequently, imaging is not optimally utilized and patients are often unnecessarily subjected to repeated CT examinations, which is undesirable. Based on the available literature and our experience, we propose certain recommendations delineating the role of imaging in the diagnosis and follow-up of such patients. The authors recognize that this is an evolving field and there may be future revisions depending on emergence of new evidence.
Keywords: Chest radiograph; TB active; chest tuberculosis (pulmonary; computed tomography; imaging recommendations; nodal and pleural).
Conflict of interest statement
Figures
References
-
- Foulds J, O’Brien R. New tools for the diagnosis of tuberculosis: The perspective of developing countries. Int J Tuberc Lung Dis. 1998;2:778–83. - PubMed
-
- Okur E, Yilmaz A, Saygi A, Selvi A, Süngün F, Oztürk E, et al. Patterns of delays in diagnosis amongst patients with smear-positive pulmonary tuberculosis at a teaching hospital in Turkey. Clin Microbiol Infect. 2006;12:90–2. - PubMed
-
- Im JG, Itoh H, Shim YS, Lee JH, Ahn J, Han MC, et al. Pulmonary tuberculosis: CT findings- early active disease and sequential change with antituberculous therapy. Radiology. 1993;186:653–60. - PubMed
-
- Jeong YJ, Lee KS. Pulmonary tuberculosis: Up-to-date imaging and management. AJR Am J Roentgenol. 2008;191:834–44. - PubMed
-
- WHO Global tuberculosis report. 2013. [Last accessed on 2014 Aug 06]. Available from: http://www.who.int/tb .
LinkOut - more resources
Full Text Sources
Other Literature Sources