

Perspectives in ultrasound-guided musculoskeletal interventions
- PMID: 26288519
- PMCID: PMC4531449
- DOI: 10.4103/0971-3026.161445
Perspectives in ultrasound-guided musculoskeletal interventions
Abstract
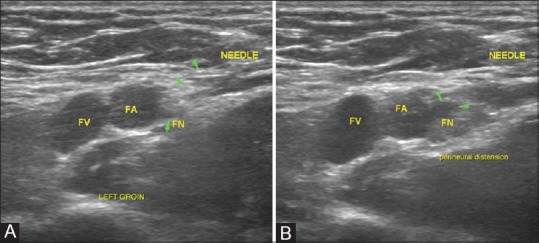
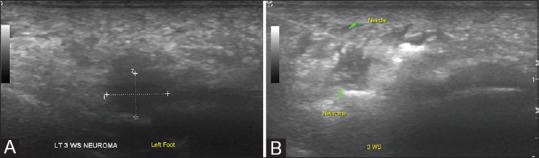
Ultrasonography (USG) is a safe, easily available, and cost-effective modality, which has the additional advantage of being real time for imaging and image-guided interventions of the musculoskeletal system. Musculoskeletal interventions are gaining popularity in sports and rehabilitation for rapid healing of muscle and tendon injuries in professional athletes, healing of chronic tendinopathies, aspiration of joint effusions, periarticular bursae and ganglia, and perineural injections in acute and chronic pain syndromes. This article aims to provide an overview of the spectrum of musculoskeletal interventions that can be done under USG guidance both for diagnostic and therapeutic purposes.
Keywords: Interventions; pain; relief; sports; ultrasound.
Conflict of interest statement
Figures
Similar articles
-
Sonography of sports injuries of the hip.Sports Health. 2014 Nov;6(6):531-8. doi: 10.1177/1941738114552801. Sports Health. 2014. PMID: 25364486 Free PMC article.
-
Ultrasound-guided interventions in the foot and ankle.Semin Musculoskelet Radiol. 2002 Jun;6(2):163-8. doi: 10.1055/s-2002-32362. Semin Musculoskelet Radiol. 2002. PMID: 12077705 Review.
-
Diagnostic and therapeutic musculoskeletal ultrasound applications of the shoulder.Muscle Nerve. 2019 Jul;60(1):1-6. doi: 10.1002/mus.26505. Epub 2019 May 11. Muscle Nerve. 2019. PMID: 31054148
-
"Sports Ultrasound", advantages, indications and limitations in upper and lower limbs musculoskeletal disorders. Review article.Int J Surg. 2018 Jun;54(Pt B):333-340. doi: 10.1016/j.ijsu.2017.11.034. Epub 2017 Nov 26. Int J Surg. 2018. PMID: 29180067 Review.
-
Existing Evidence on Ultrasound-Guided Injections in Sports Medicine.Orthop J Sports Med. 2018 Feb 22;6(2):2325967118756576. doi: 10.1177/2325967118756576. eCollection 2018 Feb. Orthop J Sports Med. 2018. PMID: 29511701 Free PMC article. Review.
Cited by
-
Using a Double Syringe Sterile System for MSK Aspiration/Injection Procedures Eliminates Risk of Iatrogenic Infection.Ther Clin Risk Manag. 2022 Oct 29;18:1029-1036. doi: 10.2147/TCRM.S372676. eCollection 2022. Ther Clin Risk Manag. 2022. PMID: 36339728 Free PMC article.
-
Ultrasound-guided therapeutic injections for neural pathology about the foot and ankle: a 4 year retrospective review.Skeletal Radiol. 2017 Jun;46(6):795-803. doi: 10.1007/s00256-017-2624-7. Epub 2017 Mar 16. Skeletal Radiol. 2017. PMID: 28303298
-
Impact of Adequate Disinfection Techniques for Ultrasound-Guided Injections in Musculoskeletal Rehabilitation: A Scoping Review.Diagnostics (Basel). 2025 Apr 5;15(7):933. doi: 10.3390/diagnostics15070933. Diagnostics (Basel). 2025. PMID: 40218283 Free PMC article. Review.
-
Ultrasound-guided peripheral nerve interventions for common pain disorders.Indian J Radiol Imaging. 2018 Jan-Mar;28(1):85-92. doi: 10.4103/ijri.IJRI_108_17. Indian J Radiol Imaging. 2018. PMID: 29692534 Free PMC article.
-
Ultrasound-guided injections in musculo-skeletal system - An overview.J Clin Orthop Trauma. 2019 Jul-Aug;10(4):669-673. doi: 10.1016/j.jcot.2019.05.013. Epub 2019 May 22. J Clin Orthop Trauma. 2019. PMID: 31316237 Free PMC article. Review.
References
-
- Louis LJ. Musculoskeletal ultrasound intervention: Principles and advances. Radiol Clin North Am. 2008;46:515–33. vi. - PubMed
-
- Stephens MB, Beutler AI, O’Connor FG. Musculoskeletal injections: A review of the evidence. Am Fam Physician. 2008;78:971–6. - PubMed
-
- Casati A, Vinciguerra F, Scarioni M, Cappelleri G, Aldegheri G, Manzoni P, et al. Lidocaine versus ropivacaine for continuous interscalene brachial plexus block after open shoulder surgery. Acta Anaesthesiol Scand. 2003;47:355–60. - PubMed
-
- Scott DB, Lee A, Fagan D, Bowler GM, Bloomfield P, Lundh R. Acute toxicity of ropivacaine compared with that of bupivacaine. Anesth Analg. 1989;69:563–9. - PubMed
-
- Glaser C, Marhofer P, Zimpfer G, Heinz MT, Sitzwohl C, Kapral S, et al. Levobupivacaine versus racemic bupivacaine for spinal anesthesia. Anesth Analg. 2002;94:194–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources