

Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas!
- PMID: 26288527
- PMCID: PMC4531457
- DOI: 10.4103/0971-3026.161467
Clinicoradiological appraisal of 'paraduodenal pancreatitis': Pancreatitis outside the pancreas!
Abstract
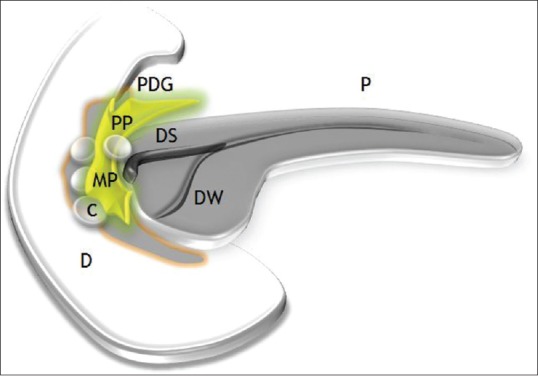
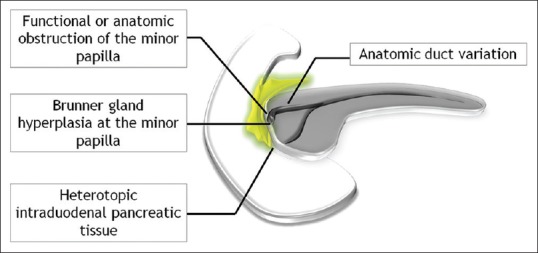
Purpose: Paraduodenal pancreatitis (PP) is a unique form of focal chronic pancreatitis that selectively involves the duodenum and aberrant pancreatic tissue located near the minor papilla (beyond the pancreas proper). The pseudotumoral nature of the disease often generates considerable clinical quandary and patient apprehension, and therefore merits a better understanding. The present study appraises the clinicoradiological manifestations of PP in 33 patients.
Materials and methods: Clinical, laboratory, and radiological manifestations of 33 patients of PP treated in gastroenterology/hepatology and hepato-pancreatico-biliary surgery units during June 2010-August 2014 were retrospectively reviewed.
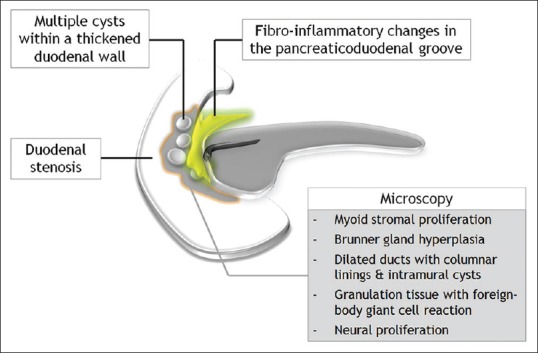
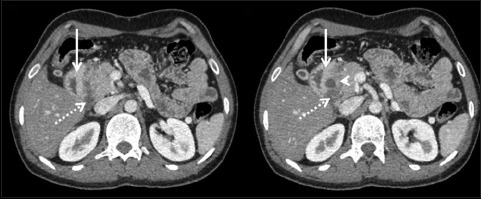
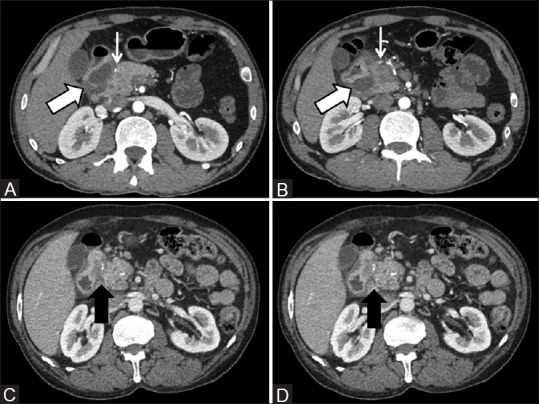
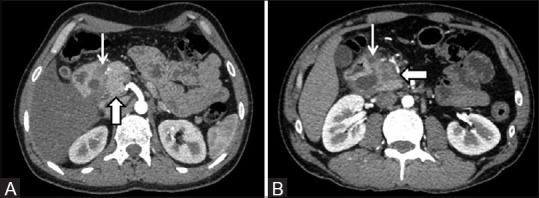
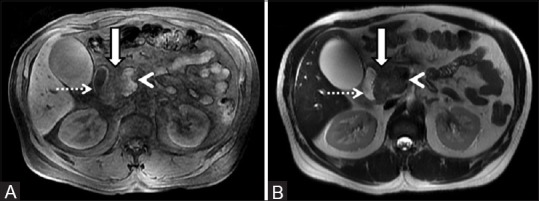
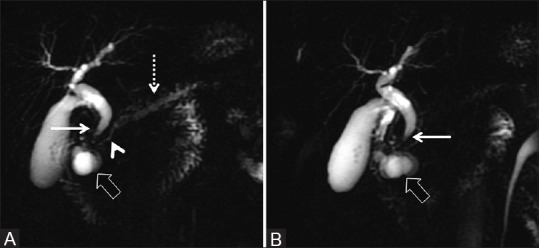
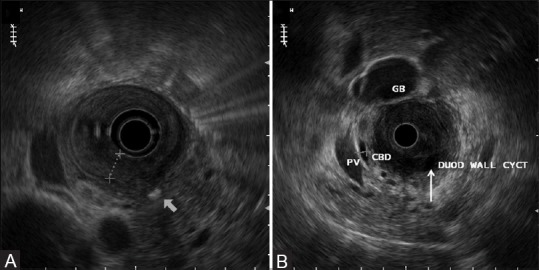
Results: All patients were young to middle-aged men (100%) with history of alcohol abuse (93.9%) and/or smoking (42.4%), who presented either with acute or gradually worsening abdominal pain (90.9%). Pancreatic enzymes and serum tumor markers remained normal or were mildly/transiently elevated. Cystic variant was detected in 57.6% (solid in 42.4%); the disease remained confined to the groove/duodenum (pure form) in 45.4%. Medial duodenal wall thickening with increased enhancement was seen in 87.87 and 81.81%, respectively, and duodenal/paraduodenal cysts were seen in 78.78%. Pancreatic calcifications and biliary stricture were seen 27.3% patients. Peripancreatic arteries were neither infiltrated nor encased.
Conclusion: PP has a discrete predilection for middle-aged men with history of longstanding alcohol abuse and/or smoking. Distinguishing imaging findings include thickening of the pancreatic side of duodenum exhibiting increased enhancement with intramural/paraduodenal cysts. This may be accompanied by plate-like scar tissue in the groove region, which may simulate groove pancreatic carcinoma. However, as opposed to carcinoma, the peripancreatic arteries are neither infiltrated nor encased, rather are medially displaced.
Keywords: Chronic pancreatitis; computed tomography; magnetic resonance imaging; pancreatitis.
Conflict of interest statement
Figures



Similar articles
-
CT imaging patterns of paraduodenal pancreatitis: a unique clinicoradiological entity.Clin Radiol. 2022 Aug;77(8):e613-e619. doi: 10.1016/j.crad.2022.04.008. Epub 2022 May 17. Clin Radiol. 2022. PMID: 35589430
-
Imaging of paraduodenal pancreatitis: A systematic review.World J Radiol. 2023 Feb 28;15(2):42-55. doi: 10.4329/wjr.v15.i2.42. World J Radiol. 2023. PMID: 36874260 Free PMC article.
-
Paraduodenal pancreatitis as diagnostic challenge: clinical and morphological features of patients with pancreatic pathology involving the pancreatic groove.Ann Gastroenterol. 2024 Nov-Dec;37(6):742-749. doi: 10.20524/aog.2024.0914. Epub 2024 Oct 20. Ann Gastroenterol. 2024. PMID: 39568705 Free PMC article.
-
Paraduodenal pancreatitis: benign and malignant mimics at MRI.Abdom Radiol (NY). 2017 Nov;42(11):2652-2674. doi: 10.1007/s00261-017-1238-9. Abdom Radiol (NY). 2017. PMID: 28660333 Review.
-
Paraduodenal pancreatitis: a clinico-pathologically distinct entity unifying "cystic dystrophy of heterotopic pancreas", "para-duodenal wall cyst", and "groove pancreatitis".Semin Diagn Pathol. 2004 Nov;21(4):247-54. doi: 10.1053/j.semdp.2005.07.005. Semin Diagn Pathol. 2004. PMID: 16273943 Review.
Cited by
-
Diagnostic value of endoscopic ultrasound in groove pancreatitis.Ann Med. 2023;55(2):2295991. doi: 10.1080/07853890.2023.2295991. Epub 2023 Dec 22. Ann Med. 2023. PMID: 38134890 Free PMC article. Review.
-
Pancreatic Neoplasms: CT Evaluation of the Uncommon Presentations of Common Lesions and Common Presentations of the Uncommon Lesions!Indian J Radiol Imaging. 2022 Aug 30;32(4):531-539. doi: 10.1055/s-0042-1754359. eCollection 2022 Dec. Indian J Radiol Imaging. 2022. PMID: 36451944 Free PMC article. Review.
-
Approach to Pancreatic Head Mass in the Background of Chronic Pancreatitis.Diagnostics (Basel). 2023 May 19;13(10):1797. doi: 10.3390/diagnostics13101797. Diagnostics (Basel). 2023. PMID: 37238280 Free PMC article. Review.
-
Pancreas-preserving duodenal resections vs pancreatoduodenectomy for groove pancreatitis. Should we revisit treatment algorithm for groove pancreatitis?World J Gastrointest Surg. 2021 Jan 27;13(1):30-49. doi: 10.4240/wjgs.v13.i1.30. World J Gastrointest Surg. 2021. PMID: 33552393 Free PMC article.
-
Groove pancreatitis: a challenging imaging diagnosis.Gland Surg. 2019 Sep;8(Suppl 3):S178-S187. doi: 10.21037/gs.2019.04.06. Gland Surg. 2019. PMID: 31559185 Free PMC article. Review.
References
-
- Arora A, Dev A, Mukund A, Patidar Y, Bhatia V, Sarin SK. Paraduodenal pancreatitis. Clin Radiol. 2014;69:299–306. - PubMed
-
- Adsay NV, Zamboni G. Paraduodenal pancreatitis: A clinico-pathologically distinct entity unifying “cystic dystrophy of heterotopic pancreas”, “para-duodenal wall cyst”, and “groove pancreatitis”. Semin Diagn Pathol. 2004;21:247–54. - PubMed
-
- Zamboni G, Capelli P, Scarpa A, Bogina G, Pesci A, Brunello E, et al. Nonneoplastic mimickers of pancreatic neoplasms. Arch Pathol Lab Med. 2009;133:439–53. - PubMed
-
- Klöppel G. Chronic pancreatitis, pseudotumors and other tumor-like lesions. Mod Pathol. 2007;20(Suppl 1):S113–31. - PubMed
-
- Casetti L, Bassi C, Salvia R, Butturini G, Graziani R, Falconi M, et al. “Paraduodenal” pancreatitis: Results of surgery on 58 consecutives patients from a single institution. World J Surg. 2009;33:2664–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous