

Prospective Analysis of More than 1,000 Patients with Rectal Carcinoma: Are There Gender-Related Differences?
- PMID: 26288586
- PMCID: PMC4513819
- DOI: 10.1159/000362680
Prospective Analysis of More than 1,000 Patients with Rectal Carcinoma: Are There Gender-Related Differences?
Abstract
Background: Since the beginning of the new millennium gender medicine has become more and more relevant. The goal has been to unveil differences in presentation, treatment response, and prognosis of men and women with regard to various diseases.
Methods: This study encompassed 1,061 patients who underwent surgery for rectal cancer at the Department of Surgery, University Medical Center Schleswig-Holstein Campus Lübeck, Germany, between January 1990 and December 2011. Prospectively documented demographic, clinical, pathological, and follow-up data were obtained. Analysis encompassed the comparison of clinical, histopathological, and oncological parameters with regard to the subcohorts of male and female patients.
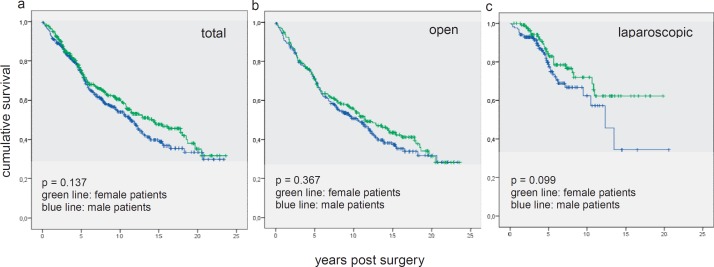
Results: No statistically significant differences could be found for clinical and histopathological parameters, location of tumor, resection with or without anastomosis, palliative or curative treatment, conversion rates, duration of surgery, and long-term survival. For the entire cohort, gender-related statistically significant differences in complications encompassed anastomotic leakage, burst abdomen, pneumonia, and urinary tract complications all of which occurred more often in men.
Conclusion: Data obtained in this study suggest that there are no gender-related differences in the oncologic surgical treatment of patients with rectal carcinoma. However, male sex seems to be a risk factor for increased early postoperative morbidity.
Hintergrund: Seit dem neuen Jahrtausend rücken geschlechtsspezifische Untersuchungen zu verschiedenen Erkrankungen zunehmend in den Fokus. Ziel ist die Erfassung von Unterschieden bezüglich Symptomen, Therapien, Therapieansprechraten und Prognosen bei Männern und Frauen.
Methoden: Diese Studie schließt 1061 Patienten mit operativer Therapie beim Rektumkarzinom in der Klinik für Allgemeine Chirurgie, Universitätsklinik Schleswig-Holstein Campus Lübeck, Deutschland, zwischen Januar 1990 und Dezember 2011 ein. Prospektiv wurden Daten zu demographischen, klinischen, pathologischen und Langzeitüberlebensraten erfasst. Die Untersuchung schließt klinische, onkologische, histopathologische und Morbiditätsdaten unter besonderer Berücksichtigung des Geschlechts ein.
Ergebnisse: Für klinische und histopathologische Parameter, Tumorlokalisationen, Resektionen mit oder ohne Anastomose, palliative oder kurative Therapien, Konversionsraten, Schnitt-Naht-Zeiten und Langzeitüberleben konnte kein geschlechtsabhängiger signifikanter Unterschied erfasst werden. Für das Gesamtkollektiv wurden geschlechtsspezifische signifikante Unterschiede zu den Parametern Anastomoseninsuffizienz, Platzbauch, Pneumonie und Harnwegskomplikationen erfasst, die allumfänglich bei Männern gehäuft auftraten.
Schlussfolgerung: Die in dieser Studie erhobenen Daten lassen den Schluss zu, dass keine geschlechtsspezifischen Unterschiede bezüglich der onkologisch-chirurgischen Behandlung beim Rektumkarzinom vorliegen. Männliches Geschlecht scheint jedoch ein Risikofaktor für eine erhöhte früh postoperative Morbidität zu sein.
Keywords: Complications; Gender; Laparoscopy; Rectal neoplasms.
Figures
References
-
- Regitz-Zagrosek V. Oertelt-Prigione S, Regitz-Zagrosek V, editors. Why do we need Gender Medicine? Sex and Gender Aspects in Clinical Medicine. London, Springer. 2012:1.
-
- Legato MJ. Cardiovascular disease in women: what's different? What's new? What's unresolved? Ann N Y Acad Sci. 1994;736:147–157. - PubMed
-
- Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352:1293–1304. - PubMed
-
- McSweeney JC, Cody M, O'Sullivan P, Elberson K, Moser DK, Garvin BJ. Women's early warning symptoms of acute myocardial infarction. Circulation. 2003;108:2619–2623. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
