

Whipple's Disease
- PMID: 26288590
- PMCID: PMC4513828
- DOI: 10.1159/000363781
Whipple's Disease
Abstract
Background: Whipple's disease (WD) is rarely the cause of a malabsorption syndrome. The disease is a chronic infection of the intestinal mucosa with the bacterium Tropheryma whipplei, which leads to a lymphostasis with an impaired absorption of the nutrition. Due to its low incidence (1:1,000,000) and the non-specific early symptoms, the disease is often diagnosed only after many years.
Methods: Based on a selective literature review and the clinical experience of the authors, the current knowledge of WD regarding pathogenesis, clinical presentation, diagnosis, and therapy are presented in this paper.
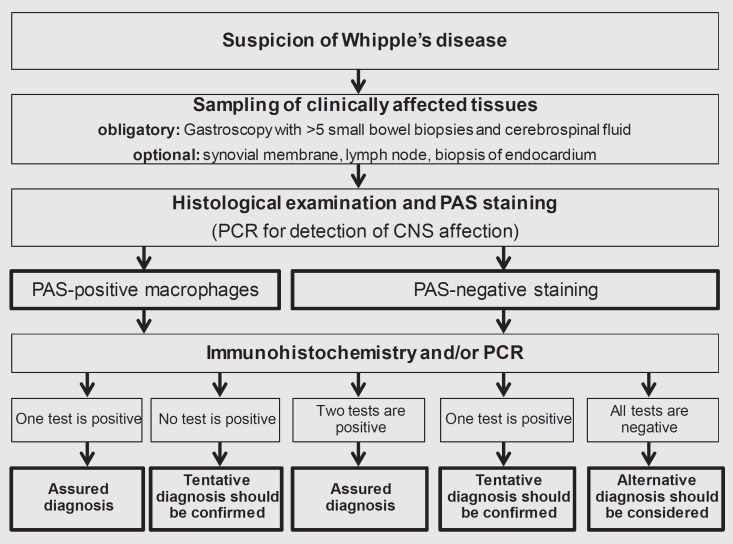
Results: Recent studies suggest that a host-specific dysfunction of the intestinal macrophages is responsible for the chronic infection with T. whipplei. Prior to patients reporting symptoms of a malabsorption syndrome (chronic diarrhea/steatorhea, weight loss), they often suffer from non-specific symptoms (polyarthralgia, fever, fatigue) for many years. Misdiagnoses such as seronegative polyarthritis are frequent. Furthermore, neurological, cardiac, ocular, or dermatological symptoms may occur. The standard method concerning diagnosis is the detection of PAS(periodic acid-Schiff)-positive macrophages in the affected tissues. Immunohistochemical staining and PCR(polymerase chain reaction)-based genetic analysis increase the sensitivity and specificity of conventional detection methods. Endoscopically, the intestinal mucosa appears edematous with lymphangiectasias, enlarged villi, and white-yellowish ring-like structures. The German treatment recommendations include a two-week intravenous induction therapy with ceftriaxone, which is followed by a three-month oral maintenance therapy with trimethoprim/sulfamethoxazole.
Conclusion: WD is rarely responsible for a malabsorption syndrome. However, if WD is not recognized, the disease can be lethal. New diagnostic methods and prospectively approved therapeutic concepts allow an adequate treatment of the patient. Due to the host-specific susceptibility to T. whipplei, a lifelong follow-up is necessary.
Hintergrund: Der Morbus Whipple kann selten die Ursache für ein Malabsorptionssyndrom sein. Ursächlich ist eine chronische Infektion der intestinalen Mukosa mit dem Bacillus Tropheryma whipplei, die zu einem Lymphstau mit einer gestörten Aufnahme der Nahrung führt. Aufgrund der geringen Inzidenz (1:1 000 000) und des unspezifischen Symptombeginns wird die Erkrankung oft erst nach vielen Jahren diagnostiziert.
Methoden: Anhand einer selektiven Literaturrecherche sowie der klinischen Erfahrungen des Autorenteams werden aktuelle Erkenntnisse der Pathogenese, der klinischen Symptomatik sowie der Diagnostik und Therapie der Erkrankung dargestellt.
Ergebnisse: Aufgrund aktueller Studien wird vermutet, dass eine wirtsspezifische Fehlfunktion der intestinalen Makrophagen ursächlich für die chronische Infektion mit T. whipplei ist. Bevor die Patienten über Symptome eines Malabsorptionssyndroms (chronische Diarrhö/Steatorrhö, Gewichtsverlust) klagen, leiden sie oft langjährig an unspezifischen Beschwerden (Polyarthralgien, Fieber, Abgeschlagenheit). Fehldiagnosen wie eine seronegative Polyarthritis sind in dieser Phase häufig. Neben klassischen Symptomen können neurologische, kardiale, okuläre oder dermatologische Symptome im Vordergrund stehen. Der Goldstandard der Diagnostik ist der Nachweis von PAS(periodic acid-Schiff)-positiven Makrophagen in den befallenen Geweben. Immunhistochemische Färbungen sowie PCR(Polymerasekettenreaktion)-basierte Genanalysen erhöhen die Sensitivität und Spezifität der gängigen Nachweismethoden. Endoskopisch wirkt die Darmmukosa ödematös, zeigt Lymphektasien und bildet weiß-gelbliche Tropfen aus. Die deutschen Therapieempfehlungen beinhalten eine zweiwöchige intravenöse Induktionstherapie mit Ceftriaxon, die von einer dreimonatigen oralen Erhaltungstherapie mit Trimethoprim/Sulfamethoxazol gefolgt wird.
Schlussfolgerung: Der Morbus Whipple ist nach wie vor selten für ein Malabsorptionssyndrom verantwortlich. Wenn die Erkrankung jedoch nicht erkannt wird, kann diese für die Betroffenen fatal enden. Neue Diagnoseverfahren sowie prospektiv geprüfte Therapiekonzepte erlauben eine adäquate Behandlung der Patienten. Aufgrund der wirtsspezifischen Suszeptibilität gegenüber T. whipplei ist jedoch eine lebenslange Nachsorge notwendig.
Keywords: Malabsorption syndrome; Tropheryma whipplei; Whipple's disease.
Figures
References
-
- Moos V, Schmidt C, Geelhaar A, Kunkel D, Allers K, Schinnerling K, Loddenkemper C, Fenollar F, Moter A, Raoult D, Ignatius R, Schneider T. Impaired immune functions of monocytes and macrophages in Whipple's disease. Gastroenterology. 2010;138:210–220. - PubMed
-
- Mönkemüller K, Fry LC, Rickes S, Malfertheiner P. Whipple's disease. Curr Infect Dis Rep. 2006;8:96–102. - PubMed
-
- Lagier J, Lepidi H, Raoult D, Fenollar F. Systemic Tropheryma whipplei clinical presentation of 142 patients with infections diagnosed or confirmed in a reference center. Medicine (Baltimore) 2010;89:337–345. - PubMed
-
- Biagi F, Trotta L, Corazza GR. Whipple's disease. Intern Emerg Med. 2012;7:209–213. - PubMed
-
- Mönkemüller K, Fry LC, von Arnim U, Neumann H, Evert M, Malfertheiner P. Whipple's disease: an endoscopic and histologic study. Digestion. 2008;77:161–165. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
