

Intravenous Thrombolysis for Acute Ischemic Stroke Within 3 Hours Versus Between 3 and 4.5 Hours of Symptom Onset
- PMID: 26288668
- PMCID: PMC4530422
- DOI: 10.1177/1941874415583116
Intravenous Thrombolysis for Acute Ischemic Stroke Within 3 Hours Versus Between 3 and 4.5 Hours of Symptom Onset
Abstract
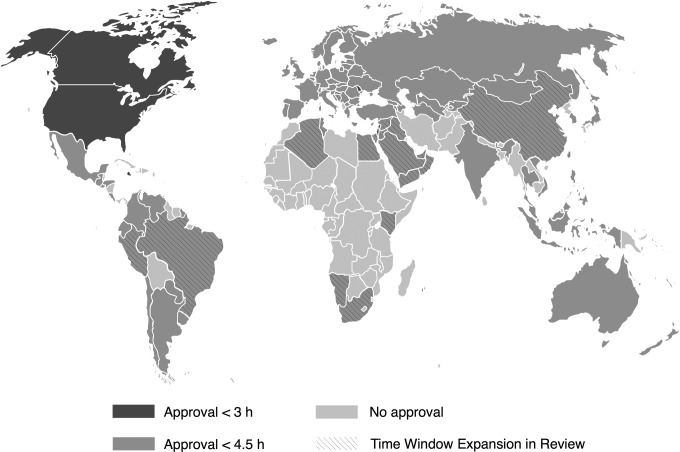
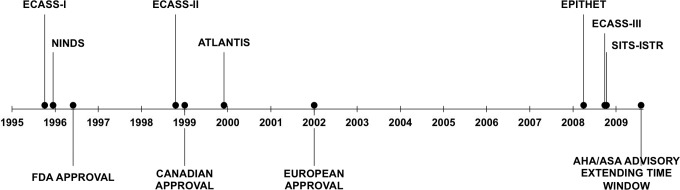
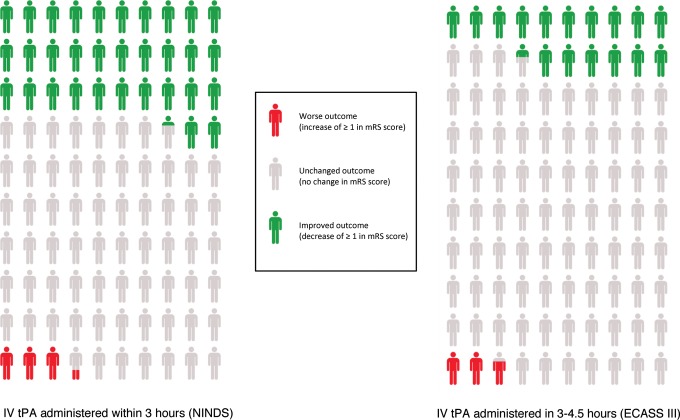
Data from randomized clinical trials have supported the safety and efficacy of intravenous tissue-type plasminogen activator (IV tPA) for acute ischemic stroke when administered within 3 hours of symptom onset, and regulatory approvals for this indication have been in place for almost 20 years. However, recent clinical trials have provided evidence that IV tPA may be safe and effective in selected patients up to 4.5 hours after symptom onset, thereby increasing the proportion of patients that may be eligible for treatment. Although professional organizations in the United States and many regulatory agencies internationally have supported this expanded time window for IV tPA, the US Food and Drug Administration has declined to approve this expanded indication and so this use of IV tPA has remained off-label in the United States. Here we review the current evidence for IV tPA in the standard and the expanded time windows and the data on current clinical practice in the United States as it relates to IV tPA treatment for acute stroke within 3 to 4.5 hours of symptom onset.
Keywords: cerebrovascular disorders; clinical specialty; clinical trials; stroke; stroke and cerebrovascular disease; techniques.
Conflict of interest statement
Figures
References
-
- Investigators CASPR (CASPR). Prioritizing interventions to improve rates of thrombolysis for ischemic stroke. Neurology. 2005;64(4):654–659. - PubMed
-
- Katzan IL. Improvement in stroke performance measures: are we moving forward or in circles? Circ Cardiovasc Qual Outcomes. 2011;4(5):493–495. - PubMed
-
- Chalouhi N, Dressler JA, Kunkel ESI, et al. Intravenous tissue plasminogen activator administration in community hospitals facilitated by telestroke service. Neurosurgery. 2013;73(4):667–671; discussion 671-672. - PubMed
-
- Hess DC, Wang S, Hamilton W, et al. REACH: clinical feasibility of a rural telestroke network. Stroke. 2005;36(9):2018–2020. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources