

Absolute Effect of Prostate Cancer Screening: Balance of Benefits and Harms by Center within the European Randomized Study of Prostate Cancer Screening
- PMID: 26289069
- PMCID: PMC4951205
- DOI: 10.1158/1078-0432.CCR-15-0941
Absolute Effect of Prostate Cancer Screening: Balance of Benefits and Harms by Center within the European Randomized Study of Prostate Cancer Screening
Erratum in
-
Correction: Absolute Effect of Prostate Cancer Screening: Balance of Benefits and Harms by Center within the European Randomized Study of Prostate Cancer Screening.Clin Cancer Res. 2016 Jul 15;22(14):3702. doi: 10.1158/1078-0432.CCR-16-1195. Clin Cancer Res. 2016. PMID: 27422205 No abstract available.
Abstract
Purpose: The balance of benefits and harms in prostate cancer screening has not been sufficiently characterized. We related indicators of mortality reduction and overdetection by center within the European Randomized Study of Prostate Cancer Screening (ERSPC).
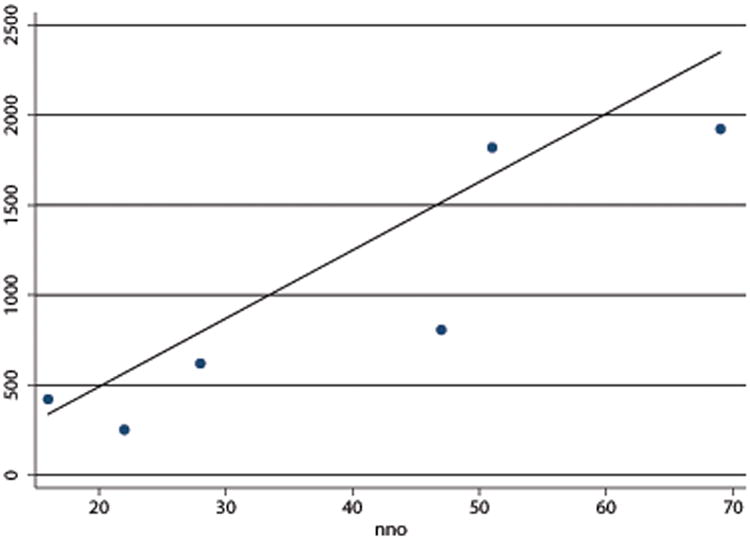
Experimental design: We analyzed the absolute mortality reduction expressed as number needed to invite (NNI = 1/absolute risk reduction; indicating how many men had to be randomized to screening arm to avert a prostate cancer death) for screening and the absolute excess of prostate cancer detection as number needed for overdetection (NNO = 1/absolute excess incidence; indicating the number of men invited per additional prostate cancer case), and compared their relationship across the seven ERSPC centers.
Results: Both absolute mortality reduction (NNI) and absolute overdetection (NNO) varied widely between the centers: NNI, 200-7,000 and NNO, 16-69. Extent of overdiagnosis and mortality reduction was closely associated [correlation coefficient, r = 0.76; weighted linear regression coefficient, β = 33; 95% confidence interval (CI), 5-62; R(2) = 0.72]. For an averted prostate cancer death at 13 years of follow-up, 12 to 36 excess cases had to be detected in various centers.
Conclusions: The differences between the ERSPC centers likely reflect variations in prostate cancer incidence and mortality, as well as in screening protocol and performance. The strong interrelation between the benefits and harms suggests that efforts to maximize the mortality effect are bound to increase overdiagnosis and might be improved by focusing on high-risk populations. The optimal balance between screening intensity and risk of overdiagnosis remains unclear.
©2015 American Association for Cancer Research.
Conflict of interest statement
Figures

References
-
- Nuovo J, Melnikow J, Chang D. Reporting number needed to treat and absolute risk reduction in randomized controlled trials. JAMA. 2002;287:2813–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
