

The effect on potential adverse drug events of a pharmacist-acquired medication history in an emergency department: a multicentre, double-blind, randomised, controlled, parallel-group study
- PMID: 26289950
- PMCID: PMC4545909
- DOI: 10.1186/s12913-015-0990-1
The effect on potential adverse drug events of a pharmacist-acquired medication history in an emergency department: a multicentre, double-blind, randomised, controlled, parallel-group study
Abstract
Background: Potential adverse drug events (PADEs) are defined as being potentially harmful unintentional medication discrepancies. Discrepancies regarding medication history (MH) often occur when a patient is being admitted to a hospital's emergency department (ED); they are clinically important and represent a significant source of data regarding adverse drug events occurring during emergency admission to hospital. This study sought to measure the impact of pharmacist-acquired MH during admission to an ED; it focused on whether a patient's current home medication regimen being available for a doctor when consulting a patient in an ED would have reduced potential adverse drug events.
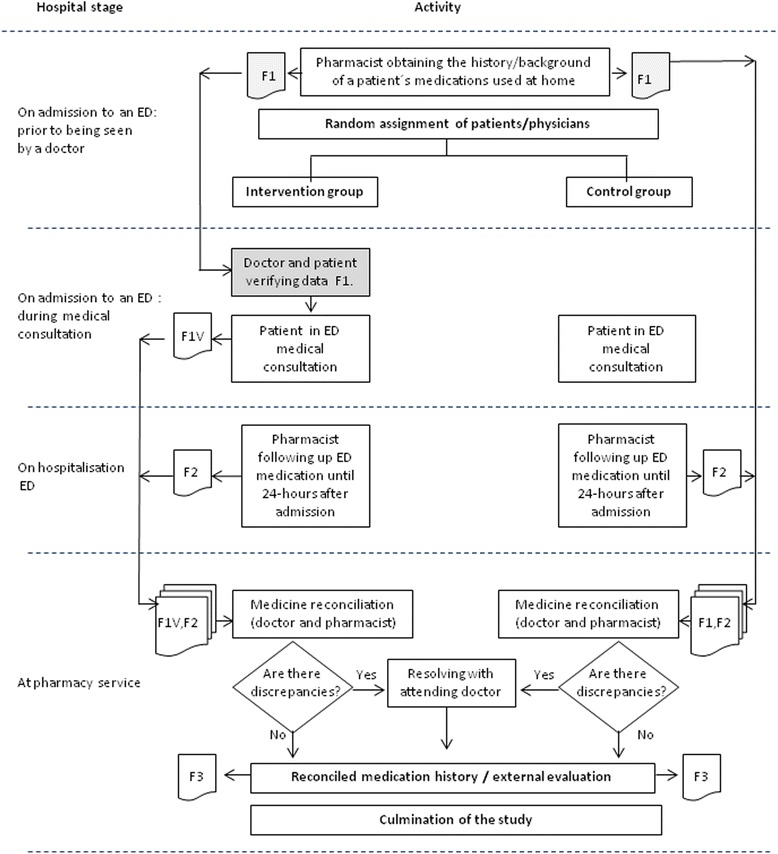
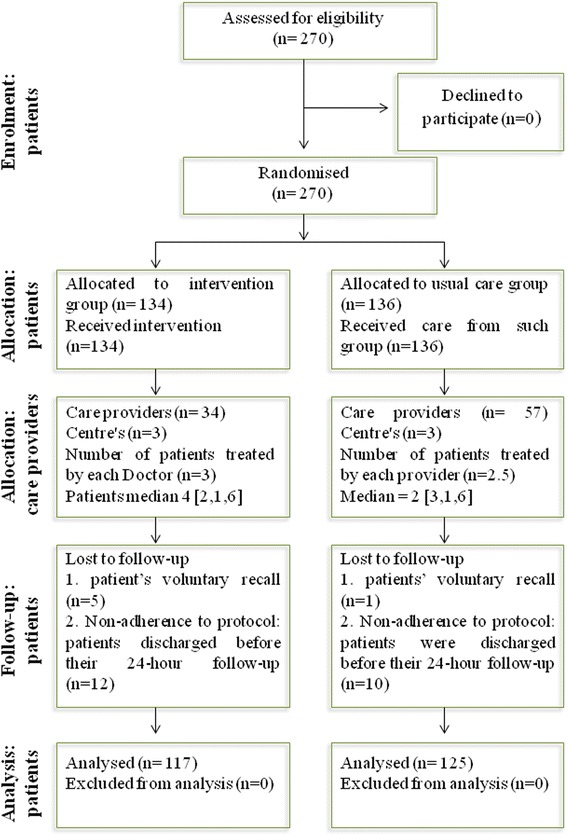
Method: A multicentre, double-blind, randomised, controlled parallel-group study was carried out at 3 large teaching hospitals in Bogota, Colombia. Two hundred and seventy patients who had been admitted to an ED were enrolled; each had a standardised, comprehensive MH interview, focusing on a patient's current home medication regimen prior to being seen by a doctor. Data recorded on the admission medication order form was available to be used by a doctor during consultation in the ED. The main outcome dealt with comparing the intervention and control groups regarding the percentage of patients having at least 1 potential adverse drug event.
Results: There were 811 PADE (3.35 per patient), 528 (65%) on the standard care arm and 283 (35%) on an intervention arm. Most PADEs were judged to have had the potential to cause moderate discomfort (42.6%), 33.4% were deemed unlikely to have caused harm and 23.9% were judged to have had the potential to cause clinical deterioration.
Conclusion: Many patients suffer potentially adverse drugs events during the transition of care from home to a hospital. Patient safety-focused medication reconciliation during admission to an ED involving a pharmacist and drawing up a history of complete medication could contribute towards reducing the risk of PADES occurring and improve follow-up of patients' medication-based therapy.
Trial registration: 28/10/2012, ISRCTN63455839.
Figures

References
-
- Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. Incidence of adverse drug events and potential adverse drug events. Implications for prevention. ADE Prevention Study Group. JAMA. 1995;274(1):29–34. - PubMed
-
- Bates DW, Spell N, Cullen DJ, Burdick E, Laird N, Petersen LA, et al. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Prevention Study Group. JAMA. 1997;277(4):307–11. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
