

The effects of somatostatin analogue therapy on pituitary tumor volume in patients with acromegaly
- PMID: 26290466
- PMCID: PMC4799266
- DOI: 10.1007/s11102-015-0677-y
The effects of somatostatin analogue therapy on pituitary tumor volume in patients with acromegaly
Abstract
Introduction: In nearly all cases, acromegaly is caused by excess GH from a pituitary adenoma, resulting in elevated circulating levels of GH and, subsequently, IGF-1. Treatment goals are to eliminate morbidity and restore the increased mortality to normal rates. Therapeutic strategies aim to minimize tumor mass and normalize GH and IGF-1 levels. Somatostatin analogues are the medical treatment of choice in acromegaly, as first-line or post-surgical therapy, and have proven efficacy in pituitary tumor volume reduction (TVR).
Methods: Here we review the effects of somatostatin analogue therapy on pituitary tumor volume in patients with acromegaly.
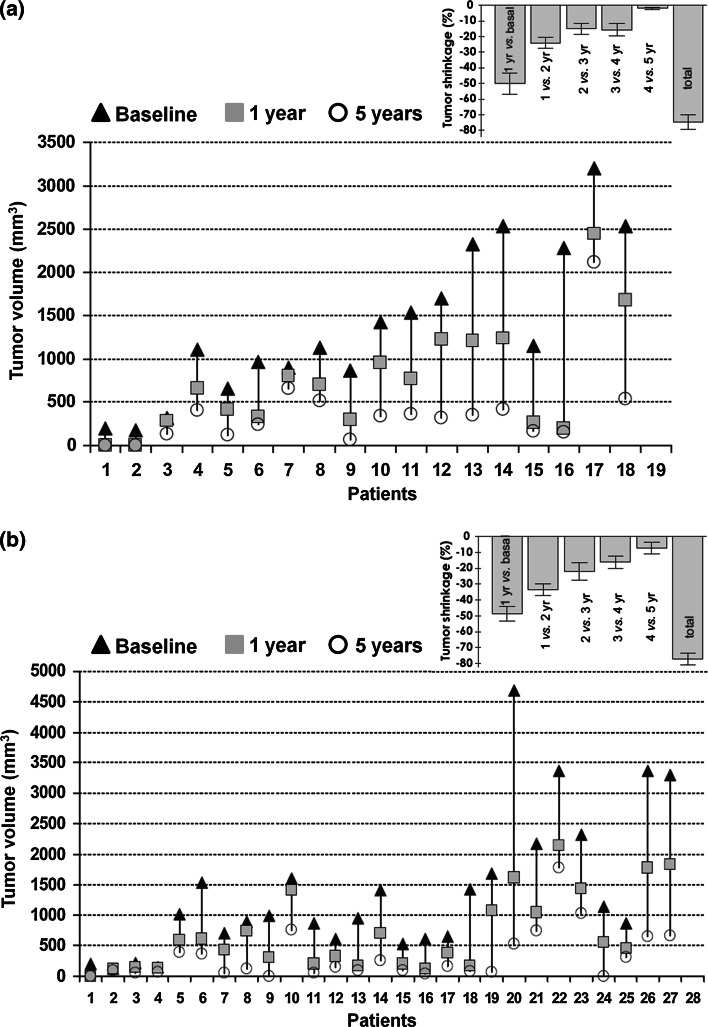
Results: TVR with somatostatin analogues may be mediated by direct anti-proliferative effects via activation of somatostatin receptors, or by indirect effects, such as angiogenesis inhibition, and is more pronounced when they are administered as first-line therapy. Various studies of first-line treatment with octreotide LAR have shown significant TVR in ≥73% of patients. First-line treatment with lanreotide Autogel has shown evidence of TVR, although more studies are needed. In a recent randomized, double-blind, 12-month trial in 358 medical-treatment-naïve acromegaly patients, significant TVR was achieved by 81% of patients administered pasireotide LAR and 77% administered octreotide LAR. Pre-operative somatostatin analogue therapy may also induce TVR and improve post-operative disease control compared with surgery alone. TVR is progressive with prolonged treatment, and decreased IGF-1 levels may be its best predictor, followed by age and degree of GH decrease. However, TVR does not always correlate with degree of biochemical control.
Conclusion: Somatostatin analogues (first- or second-line treatment) are the mainstay of medical therapy and, as first-line medical therapy, are associated with significant pituitary TVR in most patients.
Keywords: Acromegaly; Lanreotide; Octreotide; Pasireotide; Somatostatin analogue; Tumor volume.
Figures

Similar articles
-
Switching patients with acromegaly from octreotide to pasireotide improves biochemical control: crossover extension to a randomized, double-blind, Phase III study.BMC Endocr Disord. 2016 Apr 2;16:16. doi: 10.1186/s12902-016-0096-8. BMC Endocr Disord. 2016. PMID: 27039081 Free PMC article. Clinical Trial.
-
Interpreting biochemical control response rates with first-generation somatostatin analogues in acromegaly.Pituitary. 2016 Jun;19(3):235-47. doi: 10.1007/s11102-015-0684-z. Pituitary. 2016. PMID: 26519143 Free PMC article. Review.
-
Somatostatin analogues in acromegaly and gastroenteropancreatic neuroendocrine tumours: past, present and future.Endocr Relat Cancer. 2016 Dec;23(12):R551-R566. doi: 10.1530/ERC-16-0151. Epub 2016 Oct 3. Endocr Relat Cancer. 2016. PMID: 27697899 Review.
-
Long-term effects of lanreotide SR and octreotide LAR on tumour shrinkage and GH hypersecretion in patients with previously untreated acromegaly.Clin Endocrinol (Oxf). 2002 Jan;56(1):65-71. doi: 10.1046/j.0300-0664.2001.01438.x. Clin Endocrinol (Oxf). 2002. PMID: 11849248 Clinical Trial.
-
Pasireotide versus octreotide in acromegaly: a head-to-head superiority study.J Clin Endocrinol Metab. 2014 Mar;99(3):791-9. doi: 10.1210/jc.2013-2480. Epub 2014 Jan 13. J Clin Endocrinol Metab. 2014. PMID: 24423324 Free PMC article. Clinical Trial.
Cited by
-
Effectiveness and safety of pegvisomant: a systematic review and meta-analysis of observational longitudinal studies.Endocrine. 2019 Jan;63(1):18-26. doi: 10.1007/s12020-018-1729-7. Epub 2018 Aug 25. Endocrine. 2019. PMID: 30145746
-
Current and Emerging Medical Therapies in Pituitary Tumors.J Clin Med. 2022 Feb 12;11(4):955. doi: 10.3390/jcm11040955. J Clin Med. 2022. PMID: 35207228 Free PMC article. Review.
-
Systematic review and network meta-analysis assess the comparative efficacy and safety of transsphenoidal surgery for pituitary tumor.Neurosurg Rev. 2021 Feb;44(1):515-527. doi: 10.1007/s10143-020-01240-3. Epub 2020 Feb 8. Neurosurg Rev. 2021. PMID: 32036504
-
Prescription patterns of long-acting somatostatin analogues.SAGE Open Med. 2017 Mar 9;5:2050312117694795. doi: 10.1177/2050312117694795. eCollection 2017. SAGE Open Med. 2017. PMID: 28540043 Free PMC article.
-
Obesity-related gut hormones and cancer: novel insight into the pathophysiology.Int J Obes (Lond). 2021 Sep;45(9):1886-1898. doi: 10.1038/s41366-021-00865-8. Epub 2021 Jun 4. Int J Obes (Lond). 2021. PMID: 34088971
References
-
- Starke RM, Raper DM, Payne SC, Vance ML, Oldfield EH, Jane JA., Jr Endoscopic vs microsurgical transsphenoidal surgery for acromegaly: outcomes in a concurrent series of patients using modern criteria for remission. J Clin Endocrinol Metab. 2013;98(8):3190–3198. doi: 10.1210/jc.2013-1036. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
