

Enhanced recovery after surgery programs in patients undergoing hepatectomy: A meta-analysis
- PMID: 26290648
- PMCID: PMC4533053
- DOI: 10.3748/wjg.v21.i30.9209
Enhanced recovery after surgery programs in patients undergoing hepatectomy: A meta-analysis
Abstract
Aim: To evaluate the impact of enhanced recovery after surgery (ERAS) programs in comparison with traditional care on liver surgery outcomes.
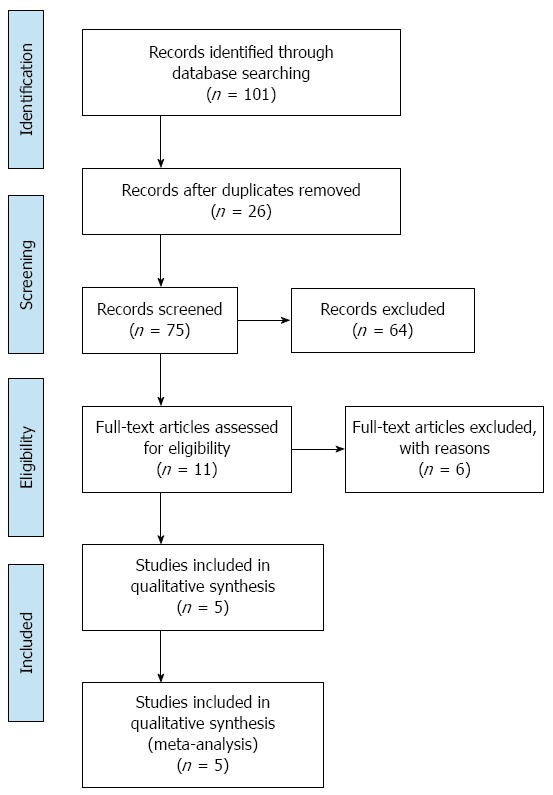
Methods: The PubMed, EMBASE, CNKI and Cochrane Central Register of Controlled Trials databases were searched for randomized controlled trials (RCTs) comparing the ERAS program with traditional care in patients undergoing liver surgery. Studies selected for the meta-analysis met all of the following inclusion criteria: (1) evaluation of ERAS in comparison to traditional care in adult patients undergoing elective open or laparoscopic liver surgery; (2) outcome measures including complications, recovery of bowel function, and hospital length of stay; and (3) RCTs. The following exclusion criteria were applied: (1) the study was not an RCT; (2) the study did not compare ERAS with traditional care; (3) the study reported on emergency, non-elective or transplantation surgery; and (4) the study consisted of unpublished studies with only the abstract presented at a national or international meeting. The primary outcomes were complications. Secondary outcomes were length of hospital stay and time to first flatus.
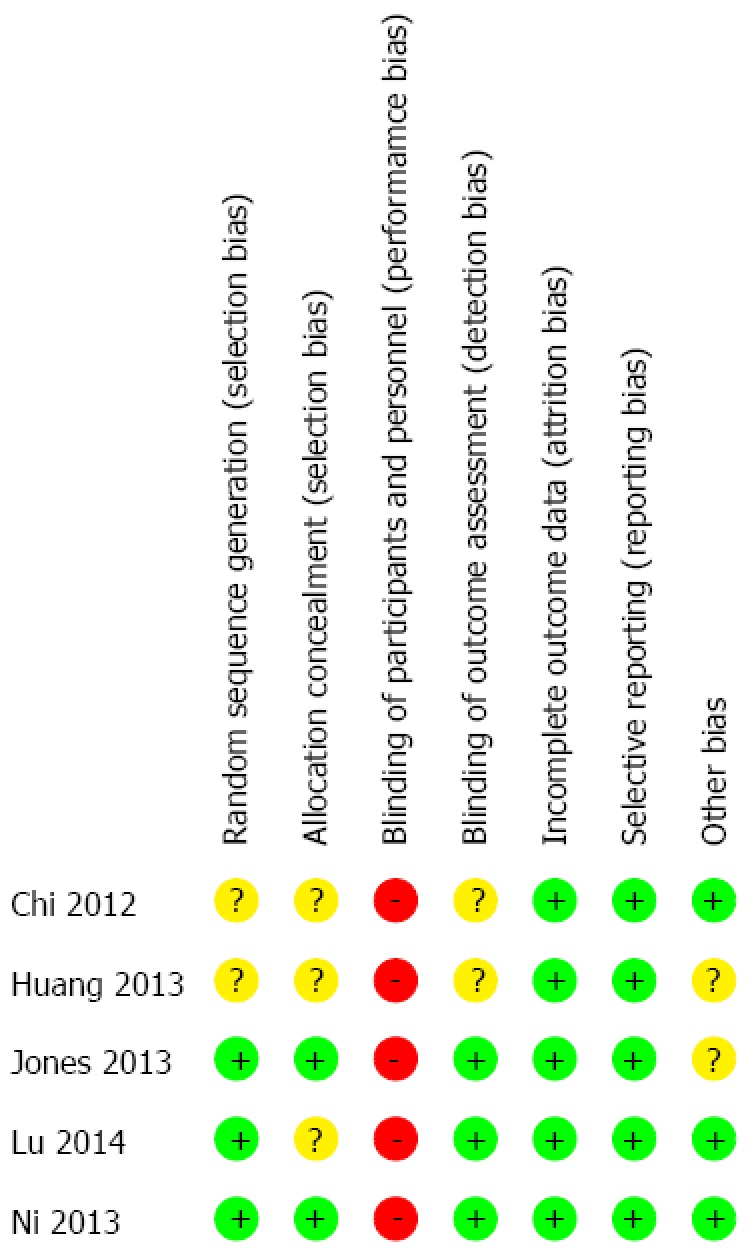
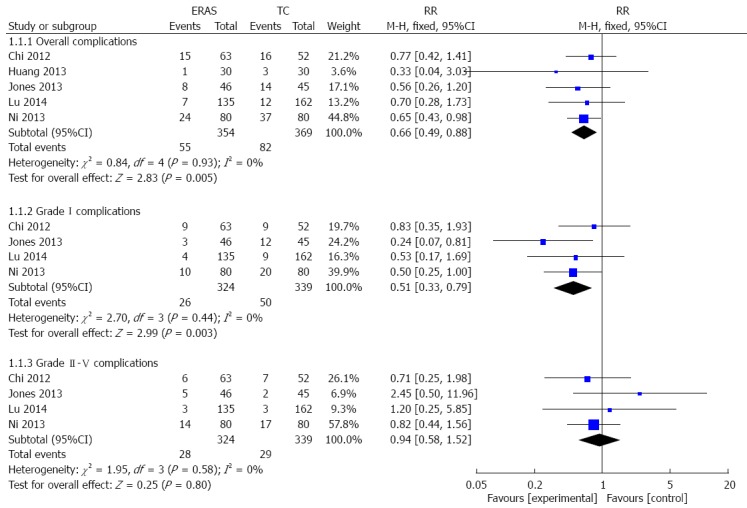
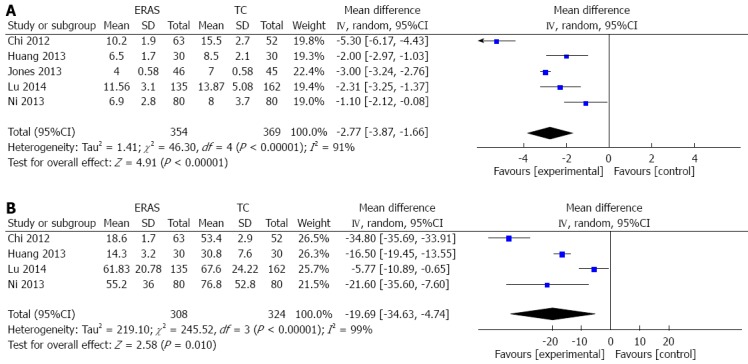
Results: Five RCTs containing 723 patients were included in the meta-analysis. In 10/723 cases, patients presented with benign diseases, while the remaining 713 cases had liver cancer. Of the five studies, three were published in English and two were published in Chinese. Three hundred and fifty-four patients were in the ERAS group, while 369 patients were in the traditional care group. Compared with traditional care, ERAS programs were associated with significantly decreased overall complications (RR = 0.66; 95%CI: 0.49-0.88; P = 0.005), grade I complications (RR = 0.51; 95%CI: 0.33-0.79; P = 0.003), and hospital length of stay [WMD = -2.77 d, 95%CI: -3.87-(-1.66); P < 0.00001]. Similarly, ERAS programs were associated with decreased time to first flatus [WMD = -19.69 h, 95%CI: -34.63-(-4.74); P < 0.0001]. There was no statistically significant difference in grade II-V complications between the two groups.
Conclusion: ERAS is a safe and effective program in liver surgery. Future studies should define the active elements to optimize postoperative outcomes for liver surgery.
Keywords: Complications; Enhanced recovery after surgery; Hospital length of stay; Liver surgery; Meta-analysis.
Figures
References
-
- Kehlet H, Slim K. The future of fast-track surgery. Br J Surg. 2012;99:1025–1026. - PubMed
-
- Kehlet H, Wilmore DW. Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg. 2008;248:189–198. - PubMed
-
- Kehlet H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth. 1997;78:606–617. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
