

Comparison of Treatment Response in Idiopathic and Connective Tissue Disease-associated Pulmonary Arterial Hypertension
- PMID: 26291092
- PMCID: PMC4642205
- DOI: 10.1164/rccm.201507-1456OC
Comparison of Treatment Response in Idiopathic and Connective Tissue Disease-associated Pulmonary Arterial Hypertension
Abstract
Rationale: Studies suggest that patients with connective tissue disease-associated pulmonary arterial hypertension (CTD-PAH) have a poorer treatment response to therapies for PAH compared with patients with idiopathic PAH (IPAH), but individual randomized controlled trials (RCTs) have been underpowered to examine differences within these subgroups.
Objectives: To compare the effect of therapy for PAH in CTD-PAH versus IPAH.
Methods: We obtained individual participant data from phase III placebo-controlled RCTs of therapies for PAH submitted to the U.S. Food and Drug Administration for drug approval. A treatment-by-diagnosis interaction term evaluated differences in treatment response between CTD-PAH and IPAH. Outcomes included change in 6-minute-walk distance (∆6MWD) from baseline to 12 weeks, clinical worsening, and all-cause mortality.
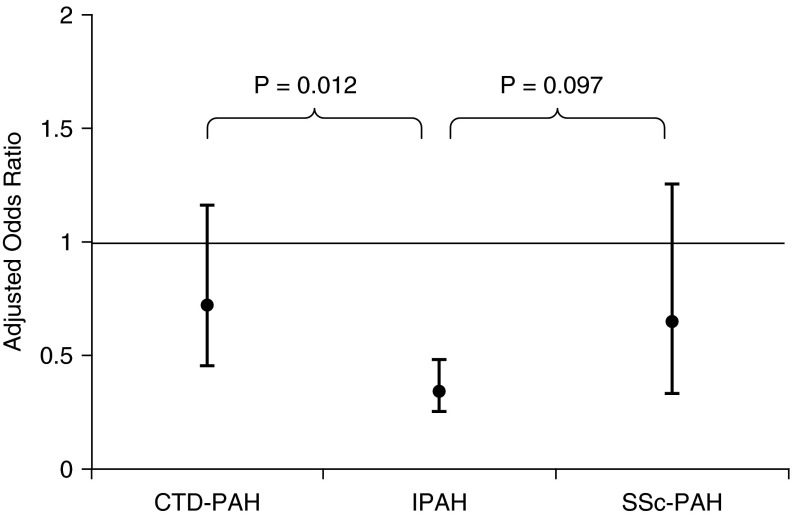
Measurements and main results: The study sample included 827 participants with CTD-PAH and 1,935 with IPAH from 11 RCTs. Patients with CTD-PAH had less improvement in 6MWD when assigned to active treatment versus placebo compared with patients with IPAH (difference in treatment effect on ∆6MWD in CTD-PAH vs. IPAH, -17.3 m; 90% confidence interval, -31.3 to -3.3; P for interaction = 0.043). Treatment was less effective in reducing the occurrence of clinical worsening in CTD-PAH versus IPAH (P for interaction = 0.012), but there was no difference in the placebo-adjusted effect of treatment on mortality (P for interaction = 0.65).
Conclusions: Treatment for PAH was less effective in CTD-PAH compared with IPAH in terms of increasing 6MWD and preventing clinical worsening. The heterogeneity of treatment response supports the need for identifying therapies that are more effective for CTD-PAH.
Keywords: clinical trial; meta-analysis; pulmonary hypertension.
Figures

References
-
- Clements PJ, Tan M, McLaughlin VV, Oudiz RJ, Tapson VF, Channick RN, Rubin LJ, Langer A Pulmonary Arterial Hypertension Quality Enhancement Research Initiative (PAH-QuERI) Investigators. The pulmonary arterial hypertension quality enhancement research initiative: comparison of patients with idiopathic PAH to patients with systemic sclerosis-associated PAH. Ann Rheum Dis. 2012;71:249–252. - PubMed
-
- Fisher MR, Mathai SC, Champion HC, Girgis RE, Housten-Harris T, Hummers L, Krishnan JA, Wigley F, Hassoun PM. Clinical differences between idiopathic and scleroderma-related pulmonary hypertension. Arthritis Rheum. 2006;54:3043–3050. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
