

Clinical Outcomes for Peripartum Cardiomyopathy in North America: Results of the IPAC Study (Investigations of Pregnancy-Associated Cardiomyopathy)
- PMID: 26293760
- PMCID: PMC5645077
- DOI: 10.1016/j.jacc.2015.06.1309
Clinical Outcomes for Peripartum Cardiomyopathy in North America: Results of the IPAC Study (Investigations of Pregnancy-Associated Cardiomyopathy)
Abstract
Background: Peripartum cardiomyopathy (PPCM) remains a major cause of maternal morbidity and mortality.
Objectives: This study sought to prospectively evaluate recovery of the left ventricular ejection fraction (LVEF) and clinical outcomes in the multicenter IPAC (Investigations of Pregnancy Associated Cardiomyopathy) study.
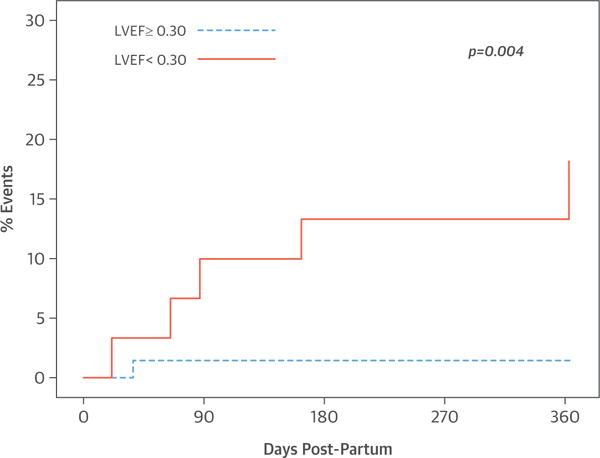
Methods: We enrolled and followed 100 women with PPCM through 1 year post-partum. The LVEF was assessed by echocardiography at baseline and at 2, 6, and 12 months post-partum. Survival free from major cardiovascular events (death, transplantation, or left ventricular [LV] assist device) was determined. Predictors of outcome, particularly race, parameters of LV dysfunction (LVEF), and remodeling (left ventricular end-diastolic diameter [LVEDD]) at presentation, were assessed by univariate and multivariate analyses.
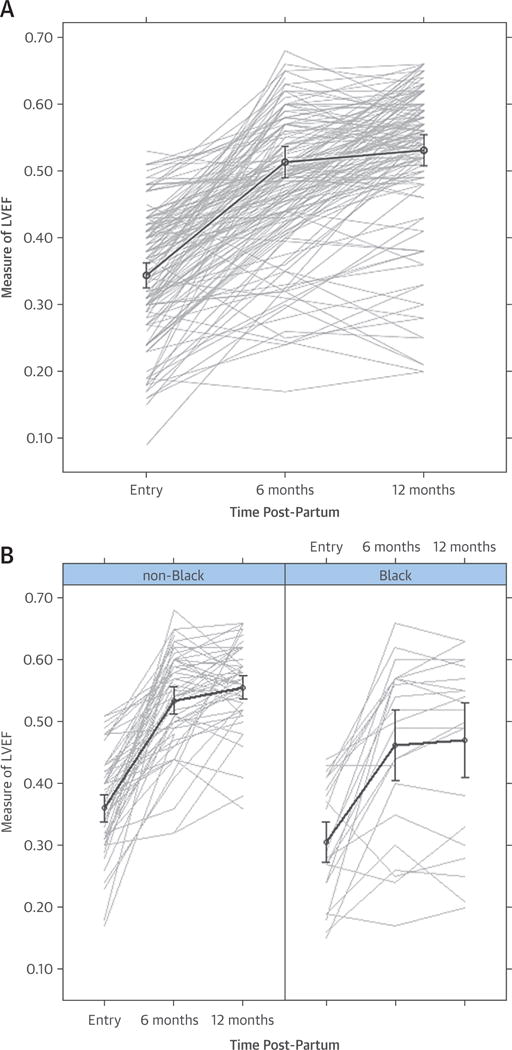
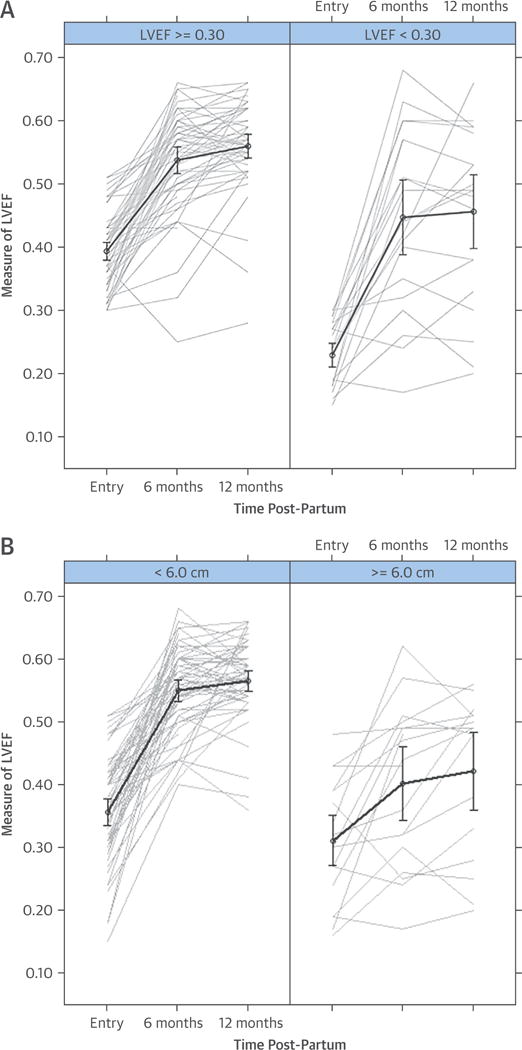
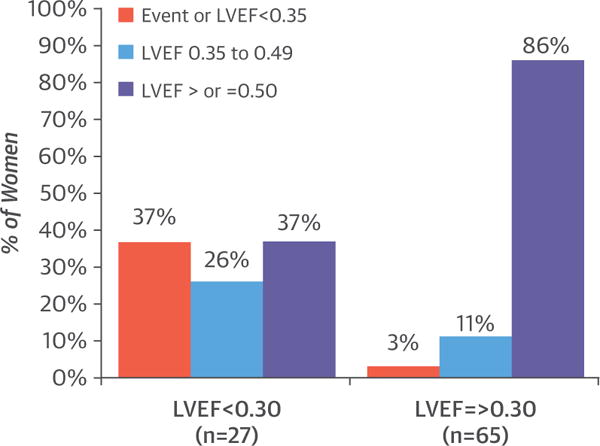
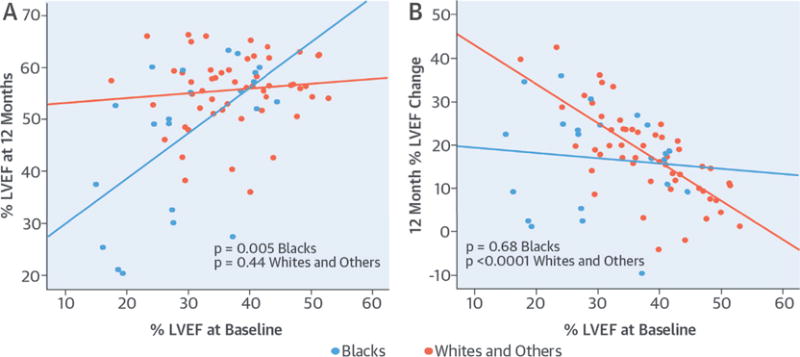
Results: The cohort was 30% black, 65% white, 5% other; the mean patient age was 30 ± 6 years; and 88% were receiving beta-blockers and 81% angiotensin-converting enzyme inhibitors or angiotensin receptor blockers. The LVEF at study entry was 0.35 ± 0.10, 0.51 ± 0.11 at 6 months, and 0.53 ± 0.10 at 12 months. By 1 year, 13% had experienced major events or had persistent severe cardiomyopathy with an LVEF <0.35, and 72% achieved an LVEF ≥0.50. An initial LVEF <0.30 (p = 0.001), an LVEDD ≥6.0 cm (p < 0.001), black race (p = 0.001), and presentation after 6 weeks post-partum (p = 0.02) were associated with a lower LVEF at 12 months. No subjects with both a baseline LVEF <0.30 and an LVEDD ≥6.0 cm recovered by 1 year post-partum, whereas 91% with both a baseline LVEF ≥0.30 and an LVEDD <6.0 cm recovered (p < 0.00001).
Conclusions: In a prospective cohort with PPCM, most women recovered; however, 13% had major events or persistent severe cardiomyopathy. Black women had more LV dysfunction at presentation and at 6 and 12 months post-partum. Severe LV dysfunction and greater remodeling at study entry were associated with less recovery. (Investigations of Pregnancy Associated Cardiomyopathy [IPAC]; NCT01085955).
Keywords: heart failure; myocardial recovery; race; remodeling.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
New Insights and Clarity for Peripartum Heart Failure and Recovery in the Modern Era.J Am Coll Cardiol. 2015 Aug 25;66(8):915-6. doi: 10.1016/j.jacc.2015.06.1326. J Am Coll Cardiol. 2015. PMID: 26293761 No abstract available.
-
Comparison of the American PPCM Registry Data With International Registries.J Am Coll Cardiol. 2016 Feb 16;67(6):733-734. doi: 10.1016/j.jacc.2015.09.112. J Am Coll Cardiol. 2016. PMID: 26868698 No abstract available.
-
Reply: Comparison of the American PPCM Registry Data With International Registries.J Am Coll Cardiol. 2016 Feb 16;67(6):734-735. doi: 10.1016/j.jacc.2015.10.094. J Am Coll Cardiol. 2016. PMID: 26868699 No abstract available.
-
Reducing the risks for relapse of heart failure in a subsequent pregnancy after peripartum cardiomyopathy?Future Cardiol. 2017 Jul;13(4):305-310. doi: 10.2217/fca-2017-0029. Epub 2017 Jun 16. Future Cardiol. 2017. PMID: 28621169 No abstract available.
References
-
- Elkayam U. Clinical characteristics of peripartum cardiomyopathy in the United States: diagnosis, prognosis, and management. J Am Coll Cardiol. 2011;58:659–70. - PubMed
-
- Mielniczuk LM, Williams K, Davis DR, et al. Frequency of peripartum cardiomyopathy. Am J Cardiol. 2006;97:1765–8. - PubMed
-
- Fett JD, Christie LG, Carraway RD, et al. Five-year prospective study of the incidence and prognosis of peripartum cardiomyopathy at a single institution. Mayo Clin Proc. 2005;80:1602–6. - PubMed
-
- Sliwa K, Förster O, Libhaber E, et al. Peripartum cardiomyopathy: inflammatory markers as predictors of outcome in 100 prospectively studied patients. Eur Heart J. 2006;27:441–6. - PubMed
-
- Brar SS, Khan SS, Sandhu GK, et al. Incidence, mortality, and racial differences in peripartum cardiomyopathy. Am J Cardiol. 2007;100:302–4. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
