

Volume-Based Peritoneal Dialysis Prescription Guide to Achieve Adequacy Targets
- PMID: 26293841
- PMCID: PMC4803365
- DOI: 10.3747/pdi.2014.00255
Volume-Based Peritoneal Dialysis Prescription Guide to Achieve Adequacy Targets
Abstract
♦
Background: The use of automated and continuous ambulatory peritoneal dialysis (APD and CAPD) prescriptions (Rxs) to achieve adequate uremic toxin and fluid removal targets is important for attaining optimal patient outcomes. One approach for predicting such Rxs is the use of kinetic modeling. ♦
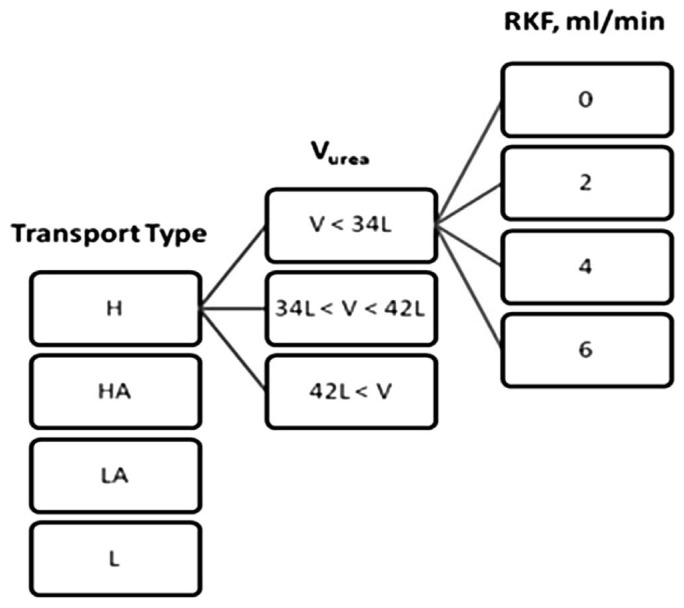
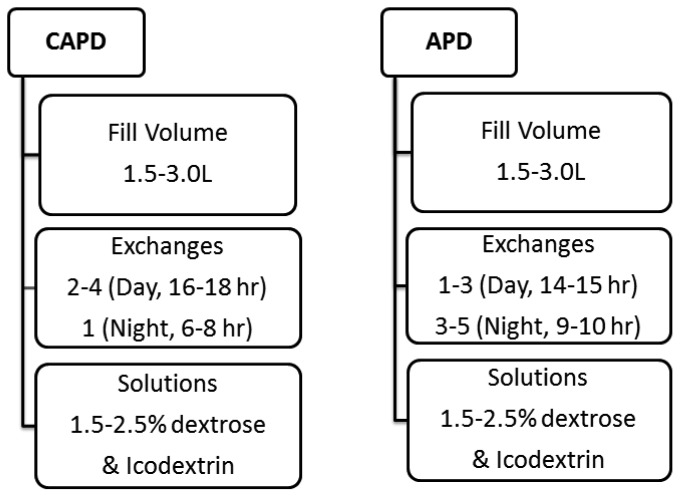
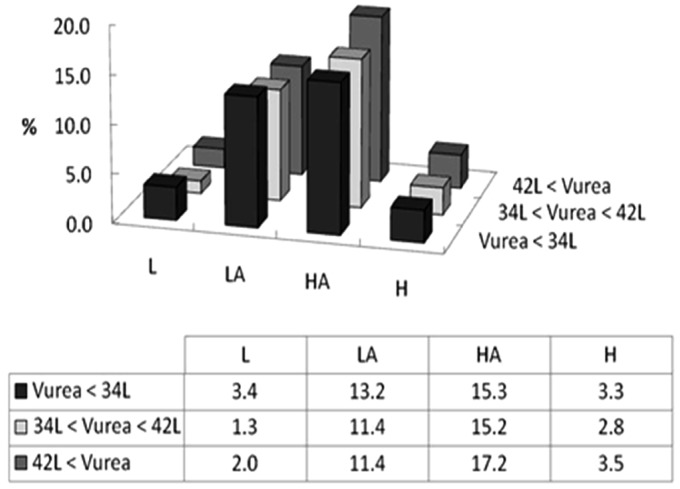
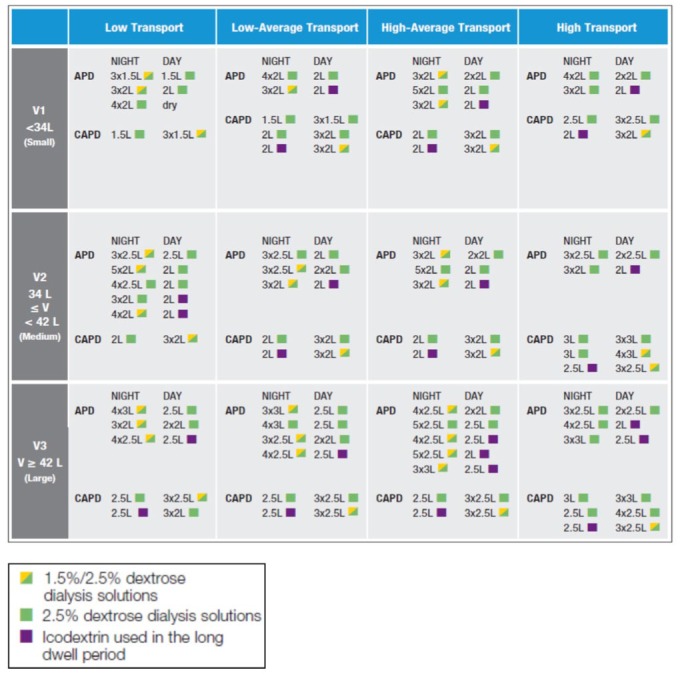
Methods: Demographic data and peritoneal membrane characteristics derived from a peritoneal equilibration test (PET) were available from 1,005 patients in North American centers who participated in a national adequacy initiative in 1999. Twelve patient subgroups were identified according to peritoneal membrane transport type and tertiles of total body water, assumed equal to urea distribution volume (Vurea). Each patient was then modeled using PD Adequest 2.0 to be treated by 12 CAPD and 34 APD Rxs using both glucose and icodextrin solutions to achieve adequacy targets of weekly urea Kt/V of 1.7 and 1 L of daily ultrafiltration (UF). Residual kidney function (RKF) was assumed to be 0, 2, 4, and 6 mL/min. Feasible peritoneal dialysis (PD) Rxs were identified where: 1) the 95% confidence limit achieved the goal of meeting the targets for urea Kt/V, daily UF, and both in 85%, 75%, and 70% of patients, respectively; 2) average PD solution dextrose concentration was < 2.5%; and 3) the number of daytime exchanges was minimized. ♦
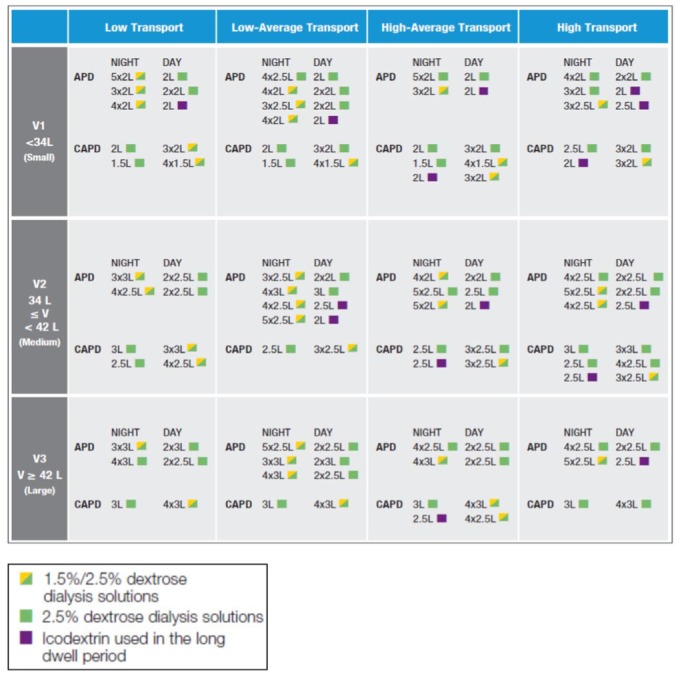
Results: Feasible PD Rxs were similar when RKF was ≥ 2 mL/min, allowing condensed recommendations based on RKF ≥ 2 mL/min or < 2 mL/min. Individuals with lower or slower membrane transport required relatively greater 24-h solution volumes to achieve adequacy targets when RKF fell below 2 mL/min. With increasing Vurea, there was disproportionately greater dependence on RKF to achieve targets. While multiple Rxs achieving urea Kt/V and daily UF goals were identified for all membrane transport types, use of icodextrin in the long dwell reduced the need for a midday exchange in APD, glucose exposure, required fill and 24-h dwell volumes, irrespective of RKF and Vurea. While these benefits were most notable in high and high-average transporters, similar results were also seen in low and low-average transporters. ♦
Conclusions: Kinetic modeling identified multiple APD and CAPD Rxs that achieved adequate uremic solute and fluid removal for patients, irrespective of RKF and Vurea. Use of icodextrin rather than glucose in the long dwell reduced the complexity of the PD regimen, total glucose exposure, and 24-h total treatment solution volumes. Irrespective of modeling, adequacy of any PD prescription should be based upon individual clinical evaluation both for volume and solute removal.
Keywords: Glucose; icodextrin; kinetic modeling; peritoneal dialysis; prescription; total body water; ultrafiltration; urea Kt/V.
Copyright © 2016 International Society for Peritoneal Dialysis.
Figures
Similar articles
-
Icodextrin Simplifies PD Therapy by Equalizing UF and Sodium Removal Among Patient Transport Types During Long Dwells: A Modeling Study.Perit Dial Int. 2016 Jan-Feb;36(1):79-84. doi: 10.3747/pdi.2013.00081. Epub 2014 Sep 2. Perit Dial Int. 2016. PMID: 25185017 Free PMC article.
-
Automated peritoneal dialysis prescriptions for enhancing sodium and fluid removal: a predictive analysis of optimized, patient-specific dwell times for the day period.Perit Dial Int. 2013 Nov-Dec;33(6):646-54. doi: 10.3747/pdi.2012.00261. Perit Dial Int. 2013. PMID: 24335125 Free PMC article.
-
A multinational clinical validation study of PD ADEQUEST 2.0. PD ADEQUEST International Study Group.Perit Dial Int. 1999 Nov-Dec;19(6):556-71. Perit Dial Int. 1999. PMID: 10641777
-
Icodextrin: a review of its use in peritoneal dialysis.Drugs. 2003;63(19):2079-105. doi: 10.2165/00003495-200363190-00011. Drugs. 2003. PMID: 12962523 Review.
-
The impact of peritoneal permeability and residual renal function on PD prescription.Perit Dial Int. 1996;16 Suppl 1:S147-52. Perit Dial Int. 1996. PMID: 8728182 Review.
Cited by
-
Economic costs of automated and continuous ambulatory peritoneal dialysis in Taiwan: a combined survey and retrospective cohort analysis.BMJ Open. 2017 Mar 21;7(3):e015067. doi: 10.1136/bmjopen-2016-015067. BMJ Open. 2017. PMID: 28325860 Free PMC article.
-
APD or CAPD: one glove does not fit all.Int Urol Nephrol. 2021 Jun;53(6):1149-1160. doi: 10.1007/s11255-020-02678-6. Epub 2020 Oct 13. Int Urol Nephrol. 2021. PMID: 33051854 Free PMC article. Review.
-
Trends in Automated Peritoneal Dialysis Prescriptions in a Large Dialysis Organization in the United States.Clin J Am Soc Nephrol. 2024 Jun 1;19(6):723-731. doi: 10.2215/CJN.0000000000000436. Epub 2024 Feb 19. Clin J Am Soc Nephrol. 2024. PMID: 38373051 Free PMC article.
References
-
- Canada-USA (CANUSA) Peritoneal Dialysis Study Group Adequacy of dialysis and nutrition in continuous peritoneal dialysis: association with clinical outcomes. J Am Soc Nephrol 1996; 7:198–207. - PubMed
-
- Paniagua R, Amato D, Vonesh E, Correa-Rotter R, Ramos A, Moran J, et al. Effects of increased peritoneal clearances on mortality rates in peritoneal dialysis: ADEMEX, a prospective, randomized, controlled trial. J Am Soc Nephrol 2002; 13:1307–20. - PubMed
-
- Lo WK, Ho YW, Li CS, Wang KS, Chan TM, Yu AW, et al. Effect of Kt/V on survival and clinical outcome in CAPD patients in a randomized prospective study. Kidney Int 2003; 64:649–56. - PubMed
-
- Dombros NV, Dratwa M, Feriani M, Gokal R, Heimbürger O, Krediet RT, et al. European best practice guidelines for peritoneal dialysis. Adequacy of peritoneal dialysis. Nephrol Dial Transplant 2005; 20(Suppl 9):ix24–7. - PubMed
-
- National Kidney Foundation KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: hemodialysis adequacy, peritoneal dialysis adequacy and vascular access. Am J Kidney Dis 2006; 48(Suppl 1):S1–232. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
