

Inter- and intra-observer variability in the classification of extracapsular extension in p16 positive oropharyngeal squamous cell carcinoma nodal metastases
- PMID: 26293844
- PMCID: PMC4875754
- DOI: 10.1016/j.oraloncology.2015.08.003
Inter- and intra-observer variability in the classification of extracapsular extension in p16 positive oropharyngeal squamous cell carcinoma nodal metastases
Abstract
Objective: Discern inter- and intra-observer variability in the classification of extracapsular extension (ECE) in p16+ oropharyngeal (OP) SCC comparing pathologists' own criteria versus those of a well-defined classification system.
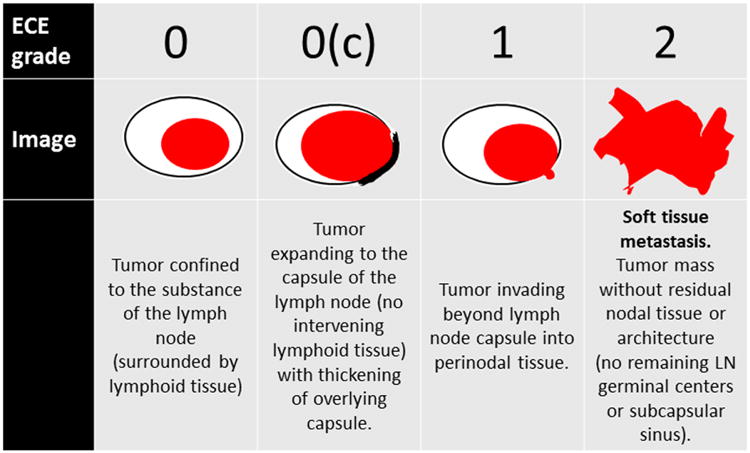
Methods: Five pathologists reviewed 50 digitally scanned nodal metastasis slides in three Rounds. Round One was by their own criteria as ECE present or absent, and Rounds Two and Three were with a defined ECE system: Grade 0 (no ECE), 0c (no ECE - thick capsule; no infiltration), 1 (ECE - cells beyond capsule), and 2 (soft tissue metastasis - cells in soft tissue without residual node). Round Three assessed intra-observer variability after an 8 month washout period.
Results: In Round One, all five agreed on only 48% of cases (n=24). Fleiss's Kappa value was 0.508 (95% CI: 0.357-0.644). For Rounds Two and Three, Grades 0 and 0c and Grades 1 and 2 were separately grouped as ECE absent or present. In Round Two, all five agreed on 68% of cases (n=34). Fleiss' Kappa was 0.635 (95% CI: 0.472-0.783), indicating statistically significantly better agreement. In Round Three, all five agreed on 64% of cases (n=32) giving a Fleiss's Kappa of 0.639. Pathologists agreed with their prior reads in approximately 90% of cases (average n=45.4, range n=42-49), an average intra-observer Cohen's Kappa of 0.8 (range: 0.68-0.95). Inter- and intra-observer variability rates for classification of soft tissue metastasis (ECE2) were substantially worse.
Conclusion: There is substantial inter-, and modest intra-, observer variability among head and neck pathologists for ECE in p16+ OPSCC, which is modestly improved by a defined system.
Keywords: Extracapsular extension; Inter-observer variability; Lymph node metastasis; Oropharyngeal squamous cell carcinoma; Soft tissue metastasis; p16.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
References
-
- Chaturvedi AK, Engels EA, Anderson WF, Gillison ML. Incidence trends for human papillomavirus-related and -unrelated oral squamous cell carcinomas in the United States. J Clin Oncol. 2008;26(4):612–9. - PubMed
-
- Sturgis EM, Cinciripini PM. Trends in head and neck cancer incidence in relation to smoking prevalence: an emerging epidemic of human papillomavirus-associated cancers? Cancer. 2007;110(7):1429–35. - PubMed
-
- Ukpo OC, Flanagan JJ, Ma XJ, Luo Y, Thorstad WL, Lewis JS., Jr High-risk human papillomavirus E6/E7 mRNA detection by a novel in situ hybridization assay strongly correlates with p16 expression and patient outcomes in oropharyngeal squamous cell carcinoma. Am J Surg Pathol. 2011;35(9):1343–50. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
