

Adrenal suppression in patients taking inhaled glucocorticoids is highly prevalent and management can be guided by morning cortisol
- PMID: 26294794
- PMCID: PMC4588051
- DOI: 10.1530/EJE-15-0608
Adrenal suppression in patients taking inhaled glucocorticoids is highly prevalent and management can be guided by morning cortisol
Abstract
Context: Up to 3% of US and UK populations are prescribed glucocorticoids (GC). Suppression of the hypothalamo-pituitary-adrenal axis with the potential risk of adrenal crisis is a recognized complication of therapy. The 250 μg short Synacthen stimulation test (SST) is the most commonly used dynamic assessment to diagnose adrenal insufficiency. There are challenges to the use of the SST in routine clinical practice, including both the staff and time constraints and a significant recent increase in Synacthen cost.
Methods: We performed a retrospective analysis to determine the prevalence of adrenal suppression due to prescribed GCs and the utility of a morning serum cortisol for rapid assessment of adrenal reserve in the routine clinical setting.
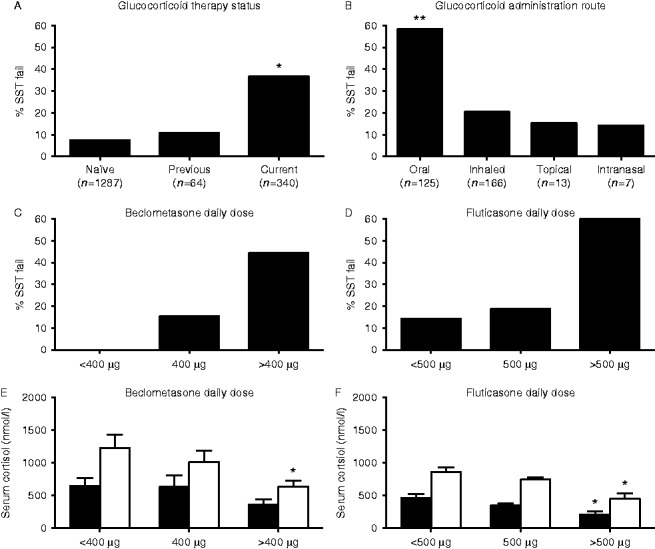
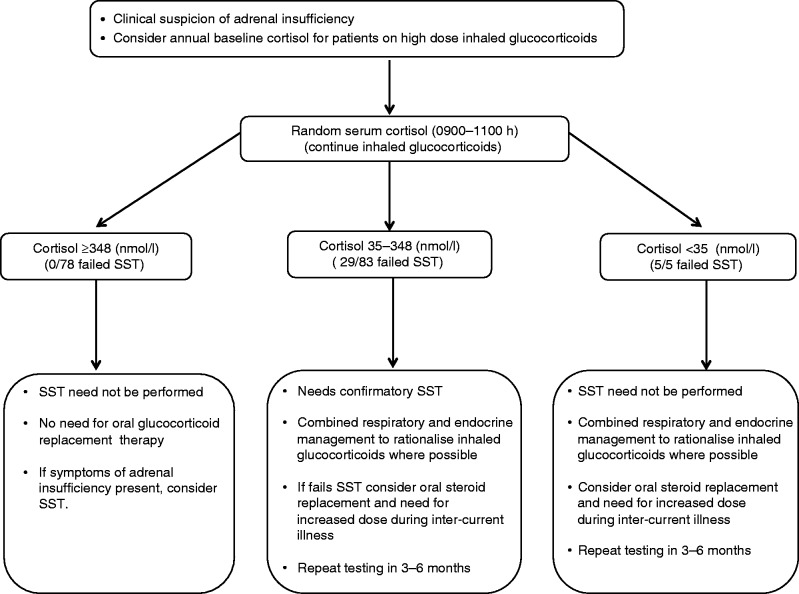
Results: In total, 2773 patients underwent 3603 SSTs in a large secondary/tertiary centre between 2008 and 2013 and 17.9% (n=496) failed the SST. Of 404 patients taking oral, topical, intranasal or inhaled GC therapy for non-endocrine conditions, 33.2% (n=134) had a subnormal SST response. In patients taking inhaled GCs without additional GC therapy, 20.5% (34/166) failed an SST and suppression of adrenal function increased in a dose-dependent fashion. Using receiver operating characteristic curve analysis in patients currently taking inhaled GCs, a basal cortisol ≥348 nmol/l provided 100% specificity for passing the SST; a cortisol value <34 nmol/l had 100% sensitivity for SST failure. Using these cut-offs, 50% (n=83) of SSTs performed on patients prescribed inhaled GCs were unnecessary.
Conclusion: Adrenal suppression due to GC treatment, particularly inhaled GCs, is common. A basal serum cortisol concentration has utility in helping determine which patients should undergo dynamic assessment of adrenal function.
© 2015 The authors.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
