

Adaptation and Evaluation of a Multi-Criteria Decision Analysis Model for Lyme Disease Prevention
- PMID: 26295344
- PMCID: PMC4546612
- DOI: 10.1371/journal.pone.0135171
Adaptation and Evaluation of a Multi-Criteria Decision Analysis Model for Lyme Disease Prevention
Abstract
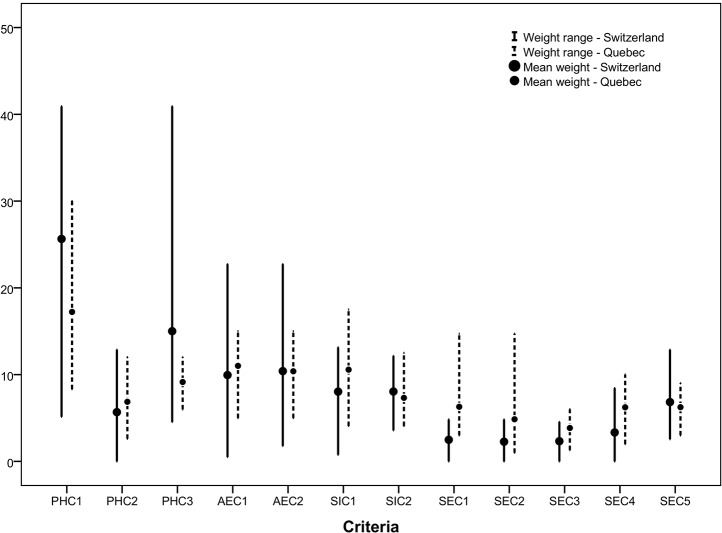
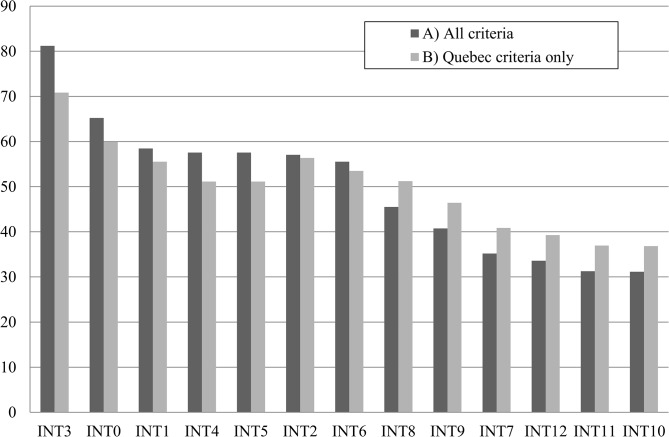
Designing preventive programs relevant to vector-borne diseases such as Lyme disease (LD) can be complex given the need to include multiple issues and perspectives into prioritizing public health actions. A multi-criteria decision aid (MCDA) model was previously used to rank interventions for LD prevention in Quebec, Canada, where the disease is emerging. The aim of the current study was to adapt and evaluate the decision model constructed in Quebec under a different epidemiological context, in Switzerland, where LD has been endemic for the last thirty years. The model adaptation was undertaken with a group of Swiss stakeholders using a participatory approach. The PROMETHEE method was used for multi-criteria analysis. Key elements and results of the MCDA model are described and contrasted with the Quebec model. All criteria and most interventions of the MCDA model developed for LD prevention in Quebec were directly transferable to the Swiss context. Four new decision criteria were added, and the list of proposed interventions was modified. Based on the overall group ranking, interventions targeting human populations were prioritized in the Swiss model, with the top ranked action being the implementation of a large communication campaign. The addition of criteria did not significantly alter the intervention rankings, but increased the capacity of the model to discriminate between highest and lowest ranked interventions. The current study suggests that beyond the specificity of the MCDA models developed for Quebec and Switzerland, their general structure captures the fundamental and common issues that characterize the complexity of vector-borne disease prevention. These results should encourage public health organizations to adapt, use and share MCDA models as an effective and functional approach to enable the integration of multiple perspectives and considerations in the prevention and control of complex public health issues such as Lyme disease or other vector-borne and zoonotic diseases.
Conflict of interest statement
Figures
Similar articles
-
Acceptability of tick control interventions to prevent Lyme disease in Switzerland and Canada: a mixed-method study.BMC Public Health. 2016 Jan 5;16:12. doi: 10.1186/s12889-015-2629-x. BMC Public Health. 2016. PMID: 26733007 Free PMC article.
-
Multi-criteria decision analysis as an innovative approach to managing zoonoses: results from a study on Lyme disease in Canada.BMC Public Health. 2013 Sep 30;13:897. doi: 10.1186/1471-2458-13-897. BMC Public Health. 2013. PMID: 24079303 Free PMC article.
-
Community-based prevention of Lyme disease and other tick-borne diseases through topical application of acaricide to white-tailed deer: background and rationale.Vector Borne Zoonotic Dis. 2009 Aug;9(4):357-64. doi: 10.1089/vbz.2009.0022. Vector Borne Zoonotic Dis. 2009. PMID: 19650729 Review.
-
Fundamental processes in the evolutionary ecology of Lyme borreliosis.Nat Rev Microbiol. 2006 Sep;4(9):660-9. doi: 10.1038/nrmicro1475. Epub 2006 Aug 7. Nat Rev Microbiol. 2006. PMID: 16894341 Review.
-
Factors associated with preventive behaviors regarding Lyme disease in Canada and Switzerland: a comparative study.BMC Public Health. 2015 Feb 25;15:185. doi: 10.1186/s12889-015-1539-2. BMC Public Health. 2015. PMID: 25884424 Free PMC article.
Cited by
-
Acceptability of tick control interventions to prevent Lyme disease in Switzerland and Canada: a mixed-method study.BMC Public Health. 2016 Jan 5;16:12. doi: 10.1186/s12889-015-2629-x. BMC Public Health. 2016. PMID: 26733007 Free PMC article.
-
A Rapid Literature Review of Multi-Criteria Decision Support Methods in the Context of One Health for All-Hazards Threat Prioritization.Front Public Health. 2022 Apr 15;10:861594. doi: 10.3389/fpubh.2022.861594. eCollection 2022. Front Public Health. 2022. PMID: 35493347 Free PMC article.
-
Spatial multi-criteria decision analysis for the selection of sentinel regions in tick-borne disease surveillance.BMC Public Health. 2024 Jan 25;24(1):294. doi: 10.1186/s12889-024-17684-x. BMC Public Health. 2024. PMID: 38267914 Free PMC article.
-
Integrated Social-Behavioral and Ecological Risk Maps to Prioritize Local Public Health Responses to Lyme Disease.Environ Health Perspect. 2018 Apr 18;126(4):047008. doi: 10.1289/EHP1943. Environ Health Perspect. 2018. PMID: 29671475 Free PMC article.
-
Development of an Index for the Inspection of Aedes aegypti Breeding Sites in Brazil: Multi-criteria Analysis.JMIR Public Health Surveill. 2021 May 10;7(5):e19502. doi: 10.2196/19502. JMIR Public Health Surveill. 2021. PMID: 33970118 Free PMC article.
References
-
- Randolph SE. Evidence that climate change has caused 'emergence' of tick-borne diseases in Europe? Int J Med Microbiol. 2004. April;293 Suppl 37:5–15. - PubMed
-
- Brownstein JS, Skelly DK, Holford TR, Fish D. Forest fragmentation predicts local scale heterogeneity of Lyme disease risk. Oecologia. 2005. December;146(3):469–75. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
