

The 2015 World Health Organization Classification of Tumors of the Thymus: Continuity and Changes
- PMID: 26295375
- PMCID: PMC4581965
- DOI: 10.1097/JTO.0000000000000654
The 2015 World Health Organization Classification of Tumors of the Thymus: Continuity and Changes
Abstract
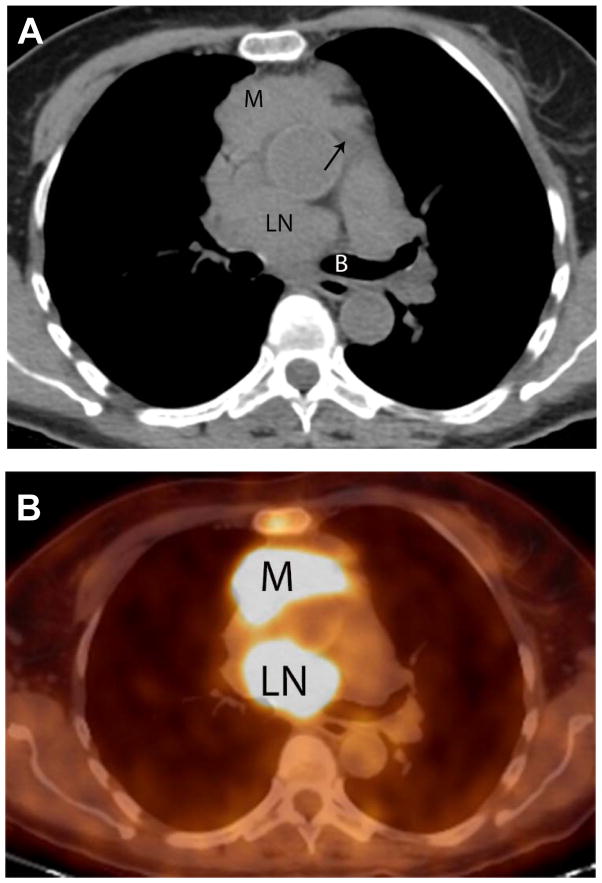
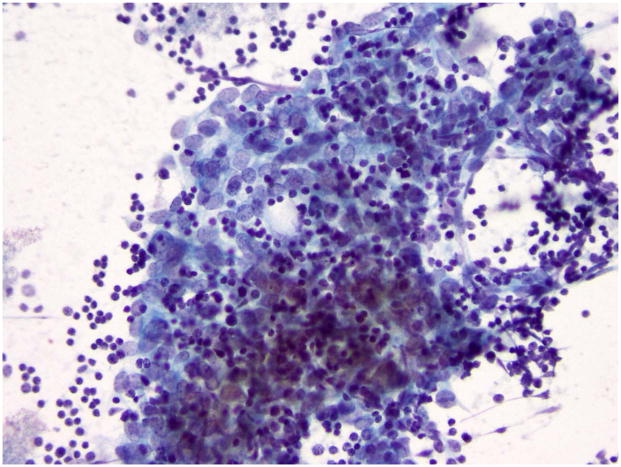
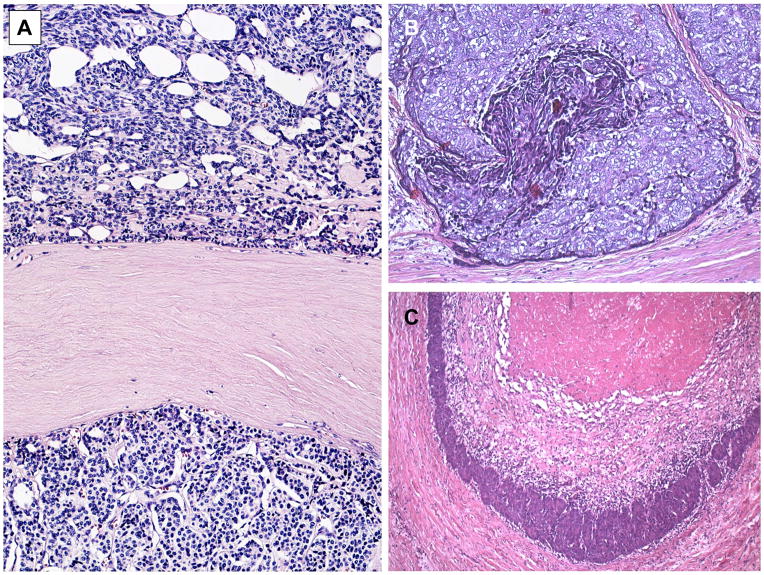
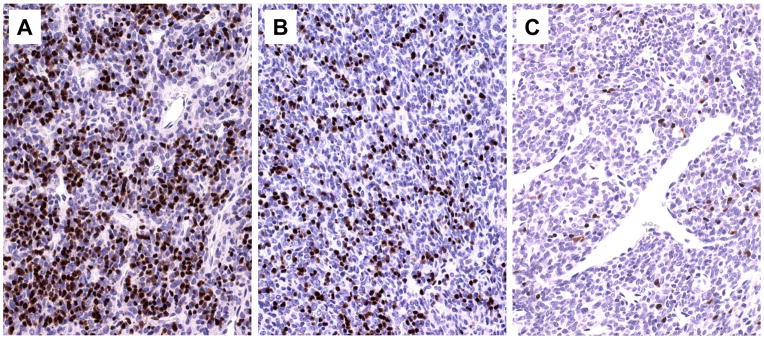
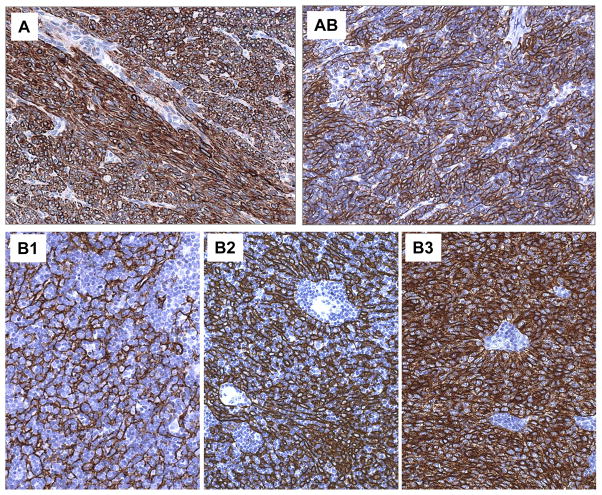
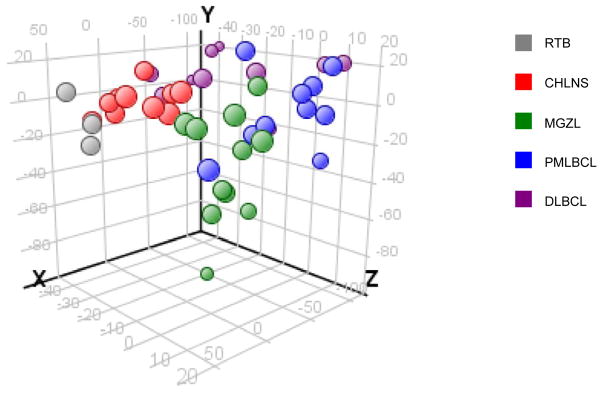
This overview of the 4th edition of the World Health Organization (WHO) Classification of thymic tumors has two aims. First, to comprehensively list the established and new tumor entities and variants that are described in the new WHO Classification of thymic epithelial tumors, germ cell tumors, lymphomas, dendritic cell and myeloid neoplasms, and soft-tissue tumors of the thymus and mediastinum; second, to highlight major differences in the new WHO Classification that result from the progress that has been made since the 3rd edition in 2004 at immunohistochemical, genetic and conceptual levels. Refined diagnostic criteria for type A, AB, B1-B3 thymomas and thymic squamous cell carcinoma are given, and it is hoped that these criteria will improve the reproducibility of the classification and its clinical relevance. The clinical perspective of the classification has been strengthened by involving experts from radiology, thoracic surgery, and oncology; by incorporating state-of-the-art positron emission tomography/computed tomography images; and by depicting prototypic cytological specimens. This makes the thymus section of the new WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart a valuable tool for pathologists, cytologists, and clinicians alike. The impact of the new WHO Classification on therapeutic decisions is exemplified in this overview for thymic epithelial tumors and mediastinal lymphomas, and future perspectives and challenges are discussed.
Figures
References
-
- Travis WD, Brambilla E, Müller-Hermelink HK, et al. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. IARC Press; 2004.
-
- Rosai J, Sobin L. Histological Typing of Tumours of the Thymus. 1999
-
- Travis WD, Brambilla E, Burke AP, et al. WHO classification of tumours of the lung, pleura, thymus and heart. IARC Press; 2015. - PubMed
-
- Strobel P, Hartmann E, Rosenwald A, et al. Corticomedullary differentiation and maturational arrest in thymomas. Histopathology. 2014;64:557–566. - PubMed
-
- Marx A, Strobel P, Badve SS, et al. ITMIG consensus statement on the use of the WHO histological classification of thymoma and thymic carcinoma: refined definitions, histological criteria, and reporting. Journal of thoracic oncology: official publication of the International Association for the Study of Lung Cancer. 2014;9:596–611. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
