

Does ultrasound provide any added value in breast contouring for radiotherapy after conserving surgery for cancer?
- PMID: 26296659
- PMCID: PMC4554322
- DOI: 10.1186/s13014-015-0487-4
Does ultrasound provide any added value in breast contouring for radiotherapy after conserving surgery for cancer?
Abstract
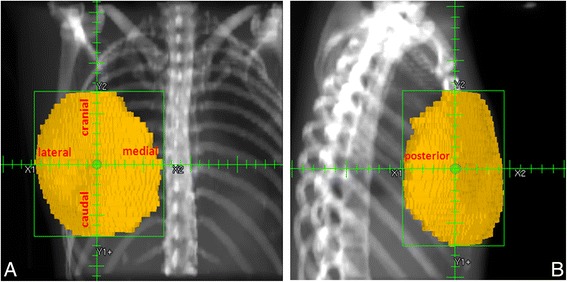
Background: Whole breast irradiation after conserving surgery for breast cancer requires precise definition of the target volume. The standard approach uses computed tomography (CT) images. However, since fatty breast and non-breast tissues have similar electronic densities, difficulties in differentiating between them hamper breast volume delineation. To overcome this limitation the breast contour is defined by palpation and then radio-opaque wire is put around it before the CT scan. To optimize assessment of breast margins in the cranial, caudal, medial, lateral and posterior directions, the present study evaluated palpation and CT and determined whether ultrasound (US) provided any added value.
Methods: Twenty consecutive patients were enrolled after they had provided informed consent to participating in this prospective study which was approved by the Regional Public Health Ethics Committee. Palpation and US defined breast margins and each contour was marked and outlined with a fine plastic wire. Breasts were then contoured on axial CT images using the breast window width (WW) and window level (WL) (401 and 750 Hounsfield Units -HU- respectively), at which setting the plastic wires were invisible. Then, the lung window function (WW 1601 HU; WL -300 HU) was inserted to visualize the plastic wires which were used as guidelines to contour the palpable and US breast volumes. As each wire had a different diameter, both volumes were easily defined on CT slices. Results were analyzed using descriptive statistics, percentage overlap and reproducibility measures (agreement and reliability).
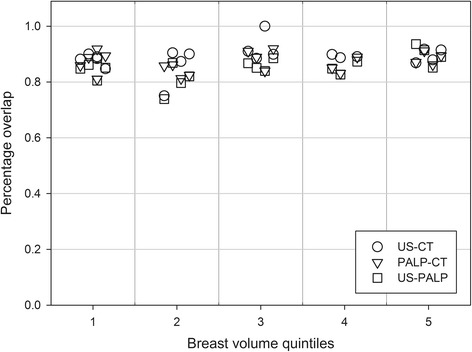
Results: Volumes: US gave the largest and palpation the smallest. Agreement was best between palpation and CT. Reliability was almost perfect in all correlations. Extensions: Cranial and posterior were highest with US and smallest with palpation. Agreement was best between palpation and CT in all extensions except the cranial. Since strong to almost perfect agreement emerged for all comparisons, reliability was high.
Conclusions: US may be useful in defining the cranial and posterior extensions, mainly when tumours are localized there. This study demonstrates that the now standard radio-opaque wires around the palpable breast may not be needed in breast contouring.
Figures



References
-
- White J, Tai A, Arthur D, Buchholz T, MacDonal S, Marks L, et al. Breast Cancer Atlas for Radiation Therapy Planning: Consensus Definitions. RTOG Radiation Therapy Oncology Group Web site. http://www.rtog.org/CoreLab/ContouringAtlases/BreastCancerAtlas.aspx. Accessed 10 Oct 2014.
-
- Nielsen MH, Berg M, Pedersen AN, Andersen K, Glavicic V, Jakobsen EH, et al. Delineation of target volumes and organs at risk in adjuvant radiotherapy of early breast cancer: national guidelines and contouring atlas by the Danish breast cancer cooperative group. Acta Oncol. 2013;52:703–10. doi: 10.3109/0284186X.2013.765064. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
