

Randomized Clinical Trial of a Sustained-Exposure Ciprofloxacin for Intratympanic Injection During Tympanostomy Tube Surgery
- PMID: 26296929
- PMCID: PMC4707869
- DOI: 10.1177/0003489415599001
Randomized Clinical Trial of a Sustained-Exposure Ciprofloxacin for Intratympanic Injection During Tympanostomy Tube Surgery
Abstract
Objective: This exploratory clinical trial evaluated the safety and clinical activity of a novel, sustained-exposure formulation of ciprofloxacin microparticulates in poloxamer (OTO-201) administered during tympanostomy tube placement in children.
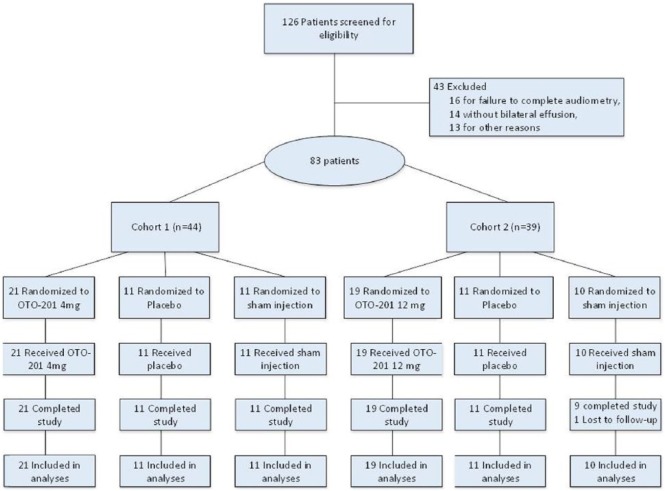
Methods: Double-blind, randomized, prospective, placebo- and sham-controlled, multicenter Phase 1b trial in children (6 months to 12 years) with bilateral middle ear effusion requiring tympanostomy tube placement. Patients were randomized to intraoperative OTO-201 (4 mg or 12 mg), placebo, or sham (2:1:1 ratio).
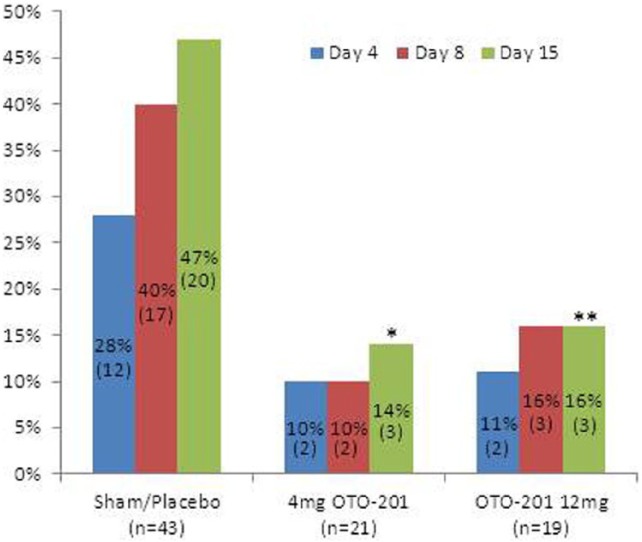
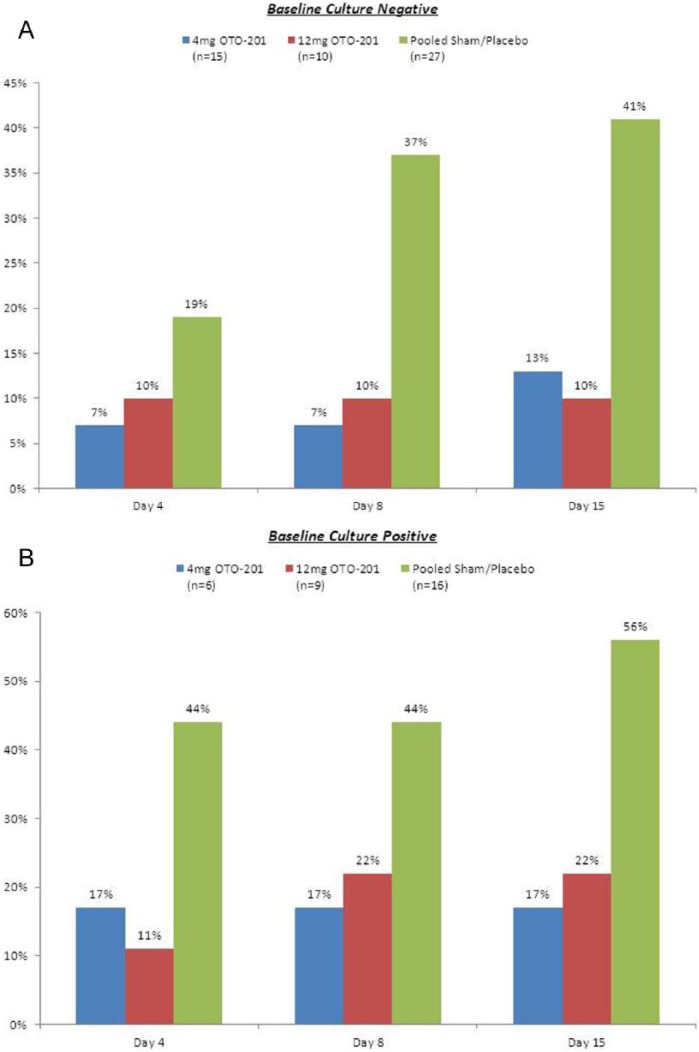
Results: Eighty-three patients (52 male/31 female; mean age, 2.80 years) were followed for safety (otoscopic exams, cultures, audiometry, and tympanometry) and clinical activity, defined as treatment failure (physician-documented otorrhea and/or otic or systemic antibiotic use ≥3 days post surgery). At baseline, 14.3% to 36.8% of children showed positive cultures of middle ear effusion samples in at least 1 ear. Through day 15, treatment failures accounted for 14.3%, 15.8%, 45.5%, and 42.9% of patients (OTO-201 4 mg, OTO-201 12 mg, placebo, and sham, respectively); treatment failure reductions for OTO-201 doses were significant compared to pooled control (P values = .023 and .043, respectively). Observed OTO-201 safety profile was indistinguishable from placebo or sham.
Conclusions: Results of this first clinical trial suggest that OTO-201 was well tolerated and shows preliminary clinical activity in treating tympanostomy tube otorrhea.
Keywords: OTO-201; ciprofloxacin; culture; middle ear effusion; otitis media; otorrhea; sustained exposure; tympanostomy tube.
© The Author(s) 2015.
Conflict of interest statement
Figures
References
-
- Owings MF, Kozak LJ. Ambulatory and inpatient procedures in the United States, 1996. Vital Health Stat. 1998;13(139):1-127. - PubMed
-
- Hellström S, Groth A, Jörgensen F, et al. Ventilation tube treatment: a systematic review of the literature. Otolaryngol Head Neck Surg. 2011;145(3):383-395. - PubMed
-
- Ah-Tye C, Paradise JL, Colborn DK. Otorrhea in young children after tympanostomy-tube placement for persistent middle-ear effusion: prevalence, incidence, and duration. Pediatrics. 2001;107(6):1251-1258. - PubMed
-
- Zipfel TE, Wood WE, Street DF, et al. The effect of topical ciprofloxacin on postoperative otorrhea after tympanostomy tube insertion. Am J Otol. 1999;20(4):416-420. - PubMed
-
- Hester TO, Jones RO, Archer SM, Haydon RC. Prophylactic antibiotic drops after tympanostomy tube placement. Arch Otolaryngol Head Neck Surg. 1995;121(4):445-448. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
