

Extending Treatment Networks in Health Technology Assessment: How Far Should We Go?
- PMID: 26297096
- PMCID: PMC4553939
- DOI: 10.1016/j.jval.2015.03.1792
Extending Treatment Networks in Health Technology Assessment: How Far Should We Go?
Abstract
Background: Network meta-analysis may require substantially more resources than does a standard systematic review. One frequently asked question is "how far should I extend the network and which treatments should I include?"
Objective: To explore the increase in precision from including additional evidence.
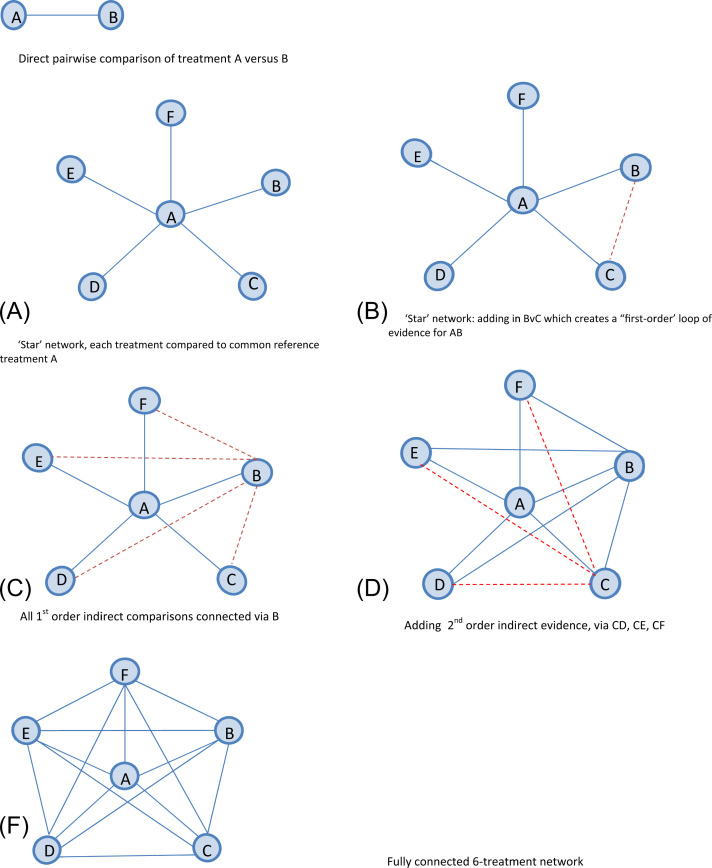
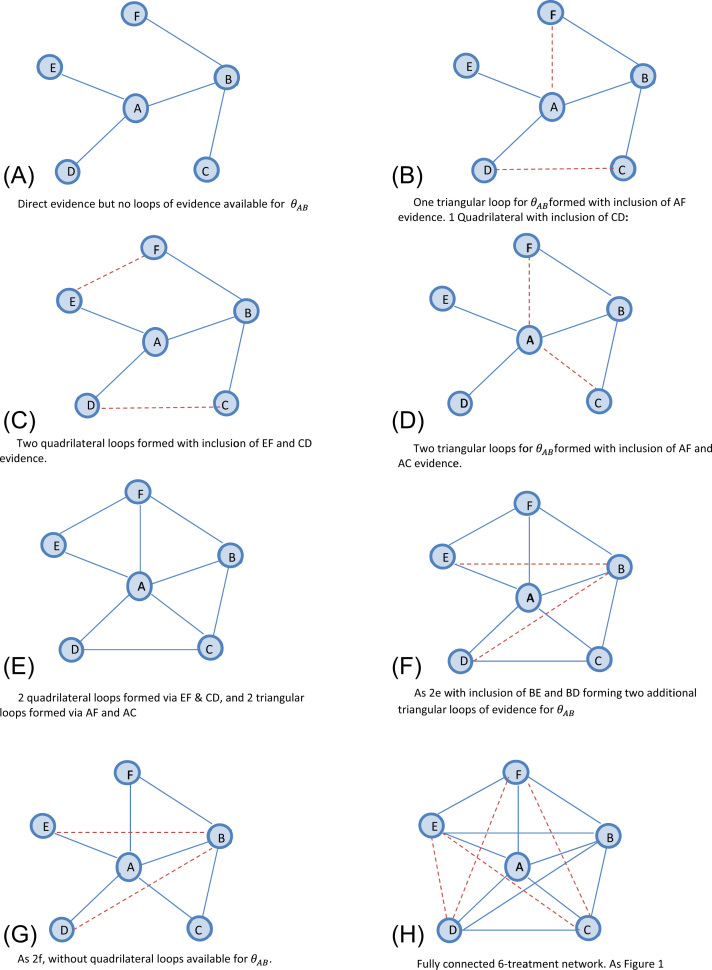
Methods: We assessed the benefit of extending treatment networks in terms of precision of effect estimates and examined how this depends on network structure and relative strength of additional evidence. We introduced a "star"-shaped network. Network complexity is increased by adding more evidence connecting treatments under five evidence scenarios. We also examined the impact of heterogeneity and absence of evidence facilitating a "first-order" indirect comparison.
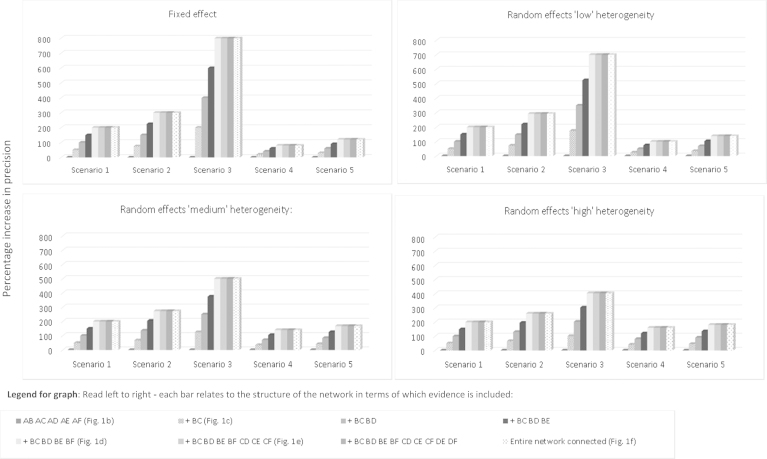
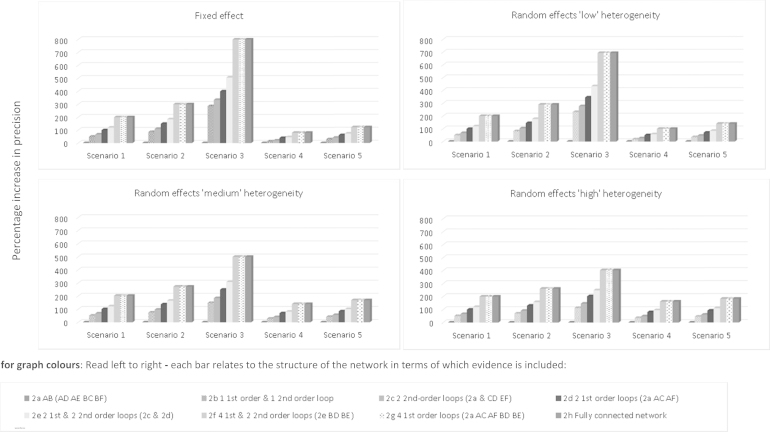
Results: In all scenarios, extending the network increased the precision of the A versus B treatment effect. Under a fixed-effect model, the increase in precision was modest when the existing direct A versus B evidence was already strong and was substantial when the direct evidence was weak. Under a random-effects model, the gain in precision was lower when heterogeneity was high. When evidence is available for all "first-order" indirect comparisons, including second-order evidence has limited benefit for the precision of the A versus B estimate. This is interpreted as a "ceiling effect."
Conclusions: Including additional evidence increases the precision of a "focal" treatment comparison of interest. Once the comparison of interest is connected to all others via "first-order" indirect evidence, there is no additional benefit in including higher order comparisons. This conclusion is generalizable to any number of treatment comparisons, which would then all be considered "focal." The increase in precision is modest when direct evidence is already strong, or there is a high degree of heterogeneity.
Keywords: comparative effectiveness; health technology assessment; literature searching; mixed treatment comparisons; network meta-analysis; systematic review.
Copyright © 2015 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- National Institute for Health and Care ExcelAU: Provide place of publication for reference 2.lence Aripiprazole for Treating Moderate to Severe Manic Episodes in Adolescents with Bipolar I Disorder. NICE technology appraisal guidance. National Institute for Health and Care Excellence. 2013
-
- Jefferson T. Ranking antidepressants. Lancet. 2009;373:1759. - PubMed
-
- Turner E., Moreno S.G., Sutton A.J. Ranking antidepressants. Lancet. 2009;373:1760. - PubMed
-
- Salanti G., Kavvoura F.K., Ioannidis J.P.A. Exploring the geometry of treatment networks. Ann Intern Med. 2008;148:544–553. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
