

Association of a 4-Tiered Classification of LV Hypertrophy With Adverse CV Outcomes in the General Population
- PMID: 26298074
- PMCID: PMC4575632
- DOI: 10.1016/j.jcmg.2015.06.007
Association of a 4-Tiered Classification of LV Hypertrophy With Adverse CV Outcomes in the General Population
Erratum in
-
Correction.JACC Cardiovasc Imaging. 2017 Dec;10(12):1537. doi: 10.1016/j.jcmg.2017.10.013. JACC Cardiovasc Imaging. 2017. PMID: 29216981 No abstract available.
Abstract
Objectives: This study was performed to determine whether a 4-tiered classification of left ventricular hypertrophy (LVH) defines subgroups in the general population that are at variable risks of adverse cardiovascular (CV) outcomes.
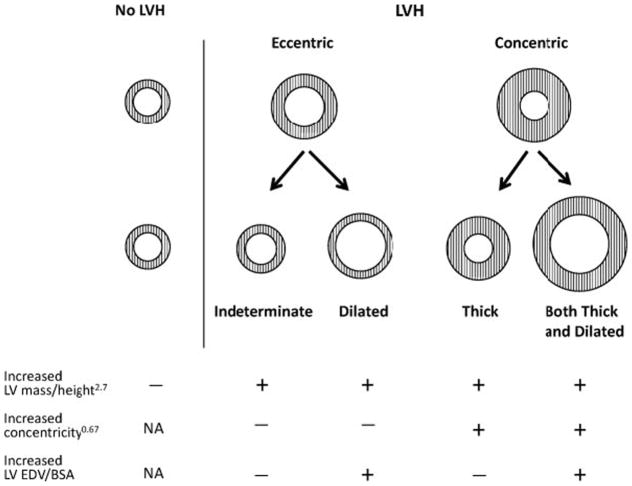
Background: We recently proposed a 4-tiered classification of LVH where eccentric LVH is subdivided into "indeterminate hypertrophy" and "dilated hypertrophy" and concentric LVH into "thick hypertrophy" and "both thick and dilated hypertrophy," based on the presence of increased left ventricular (LV) end-diastolic volume.
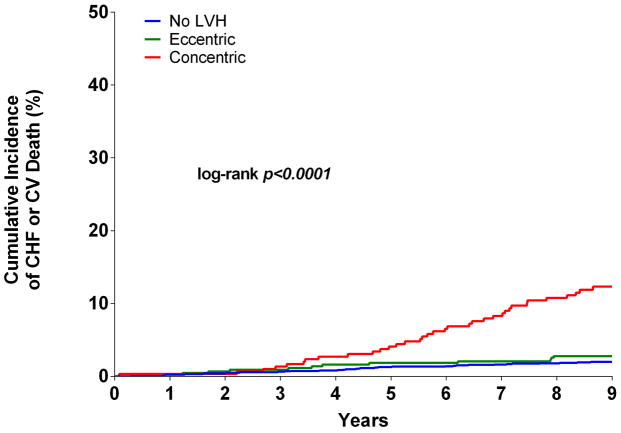
Methods: Participants from the Dallas Heart study who underwent cardiac magnetic resonance and did not have LV dysfunction or a history of heart failure (HF) (n = 2,458) were followed for a median of 9 years for the primary outcome of HF or CV death. Multivariable Cox proportional hazards models were used to adjust for age, sex, African-American race, hypertension, diabetes, and history of CV disease.
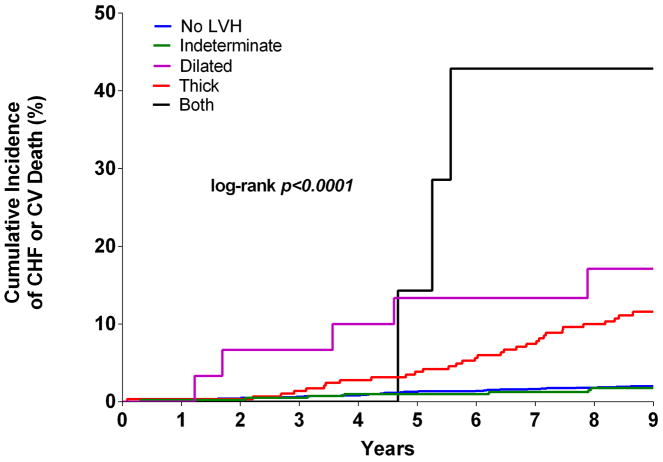
Results: In the cohort, 70% had no LVH, 404 (16%) had indeterminate hypertrophy, 30 (1%) had dilated hypertrophy, 289 (12%) had thick hypertrophy, and 7 (0.2%) had both thick and dilated hypertrophy. The cumulative incidence of HF or CV death was 2% with no LVH, 1.7% with indeterminate, 16.7% with dilated, 11.1% with thick, and 42.9% with both thick and dilated hypertrophy (log-rank p < 0.0001). Compared with participants without LVH, those with dilated (hazard ratio [HR]: 7.3; 95% confidence interval [CI]: 2.8 to 18.8), thick (HR: 2.4; 95% CI: 1.4 to 4.0), and both thick and dilated (HR: 5.8; 95% CI: 1.7 to 19.5) hypertrophy remained at increased risk for HF or CV death after multivariable adjustment, whereas the group with indeterminate hypertrophy was not (HR: 0.9; 95% CI: 0.4 to 2.2).
Conclusions: In the general population, the 4-tiered classification system for LVH stratified LVH into subgroups with differential risk of adverse CV outcomes.
Keywords: cardiac magnetic resonance; heart failure; hypertrophy; left ventricular geometry; troponin.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Shape of LVH in Hypertension: What Does it Tell Us?JACC Cardiovasc Imaging. 2015 Sep;8(9):1042-1044. doi: 10.1016/j.jcmg.2015.08.002. JACC Cardiovasc Imaging. 2015. PMID: 26381766 No abstract available.
References
-
- Drazner MH, Rame JE, Marino EK, et al. Increased left ventricular mass is a risk factor for the development of a depressed left ventricular ejection fraction within five years: the Cardiovascular Health Study. J Am Coll Cardiol. 2004;43:2207–15. - PubMed
-
- Gottdiener JS, Arnold AM, Aurigemma GP, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol. 2000;35:1628–37. - PubMed
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990;322:1561–6. - PubMed
-
- Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the american society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. 2015;28:1–39. e14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
