

Gender and outcomes after primary prevention implantable cardioverter-defibrillator implantation: Findings from the National Cardiovascular Data Registry (NCDR)
- PMID: 26299231
- PMCID: PMC4768728
- DOI: 10.1016/j.ahj.2015.02.025
Gender and outcomes after primary prevention implantable cardioverter-defibrillator implantation: Findings from the National Cardiovascular Data Registry (NCDR)
Abstract
Background: Clinical trials have demonstrated the benefit of implantable cardioverter-defibrillators (ICDs) for the primary prevention of sudden cardiac death in selected high-risk individuals. Because of small numbers of women enrolled in these trials, outcomes for women after hospital discharge have not been well described. We compared procedure-related complications and outcomes after hospital discharge between men and women undergoing single- or dual-chamber ICD implantation for primary prevention.
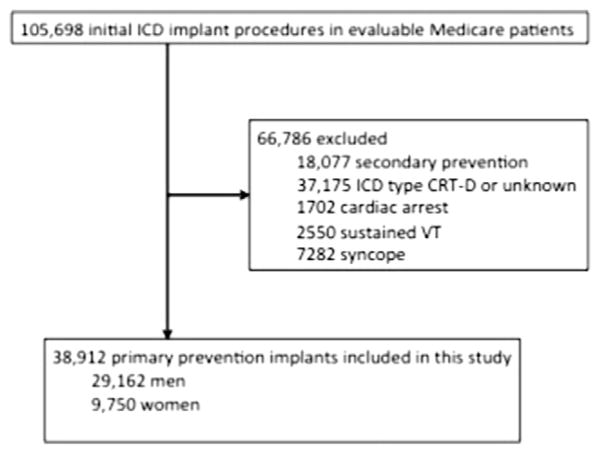
Methods: In patients 65 years or older with Medicare fee-for-service coverage, we identified 38,912 initial implants (25% women) who received single- or dual-chamber ICDs for primary prevention between January 2006 and December 2009 in the NCDR and evaluated gender differences in outcomes.
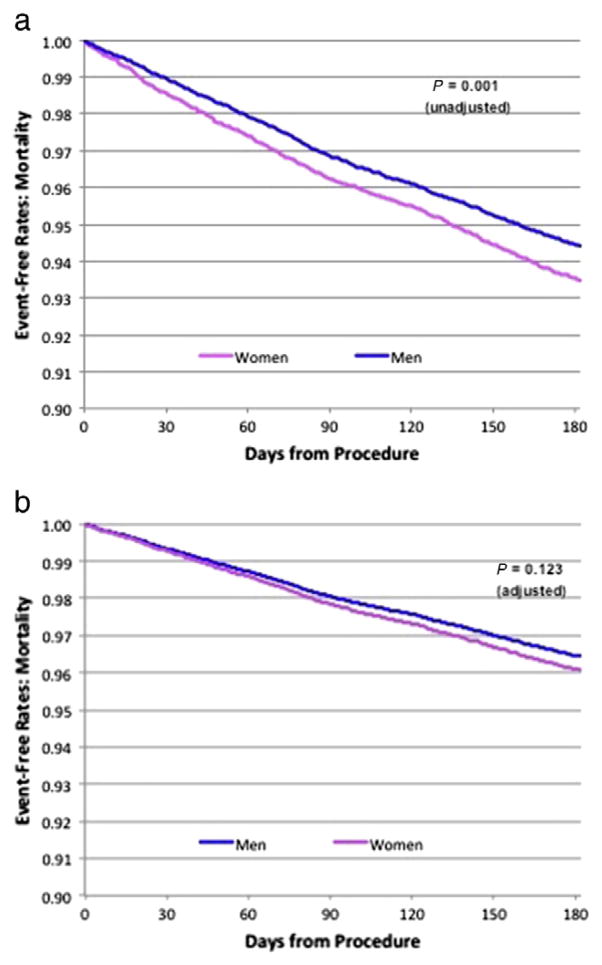
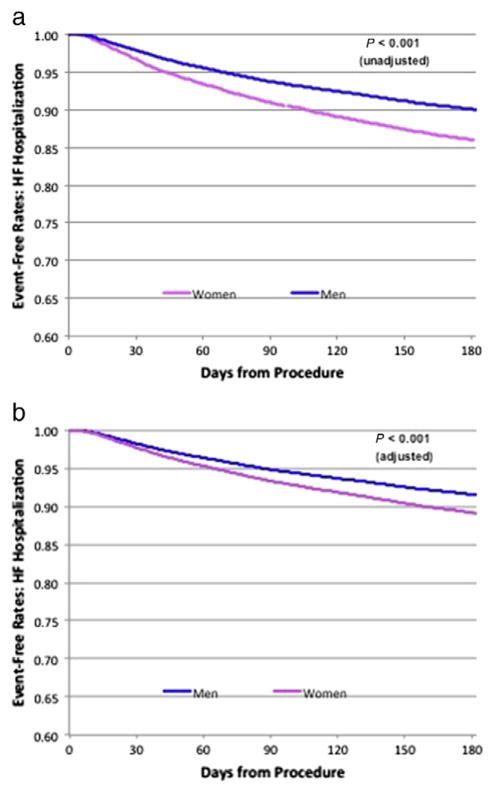
Results: Women had greater comorbidity and more advanced heart failure (HF) at the time of ICD implantation than did men. Device-related complications, death at 6 months, all-cause readmissions, and HF readmissions at 6 months were significantly more common in women (7.2% vs 4.8%, 6.5% vs 5.6%, 37.2% vs 31.7%, and 14.0% vs 10.0% respectively; P < .001 for all). Women continued to have higher odds of procedural complications (odds ratio [OR] 1.39, 95% CI 1.26-1.53, P < .001), 6-month all-cause readmission (OR 1.22, 95% CI 1.16-1.28, P < .001), and 6-month HF readmission (OR 1.32, 95% CI 1.23-1.42, P < .001), with a trend toward higher 6-month mortality (OR 1.08, 95% CI 0.98-1.20, P = .123), compared with men, after adjusting for differences in baseline characteristics and device type (single vs dual chamber).
Conclusions: Among older patients receiving ICDs for primary prevention in clinical practice, women experience worse outcomes than do men. Reasons for gender differences in outcomes are poorly understood and require further investigation.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Primary prevention implantable cardioverter defibrillators in women: More questions than answers.Am Heart J. 2015 Aug;170(2):197-9. doi: 10.1016/j.ahj.2015.04.005. Epub 2015 Apr 11. Am Heart J. 2015. PMID: 26299213 No abstract available.
References
-
- Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996;335:1933–40. - PubMed
-
- Moss AJ, Zareba W, Hall J, et al. Prophylactic Implantation of a Defibrillator in Patients With Myocardial Infarction and Reduced Ejection Fraction. N Engl J Med. 2002;346:877–83. - PubMed
-
- Buxton AE, Lee KL, Fisher JD, et al. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med. 1999;341:1882–90. - PubMed
-
- Kadish A, Dyer A, Daubert JP, et al. for the Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigators. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350:2151–8. - PubMed
-
- Bardy GH, Lee KL, Mark DB, et al. for the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
