

Gains in cognition through combined cognitive and physical training: the role of training dosage and severity of neurocognitive disorder
- PMID: 26300772
- PMCID: PMC4528297
- DOI: 10.3389/fnagi.2015.00152
Gains in cognition through combined cognitive and physical training: the role of training dosage and severity of neurocognitive disorder
Abstract
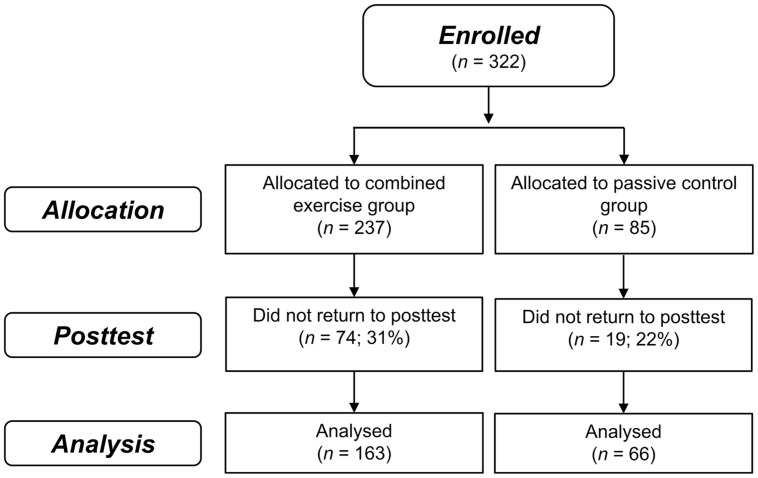
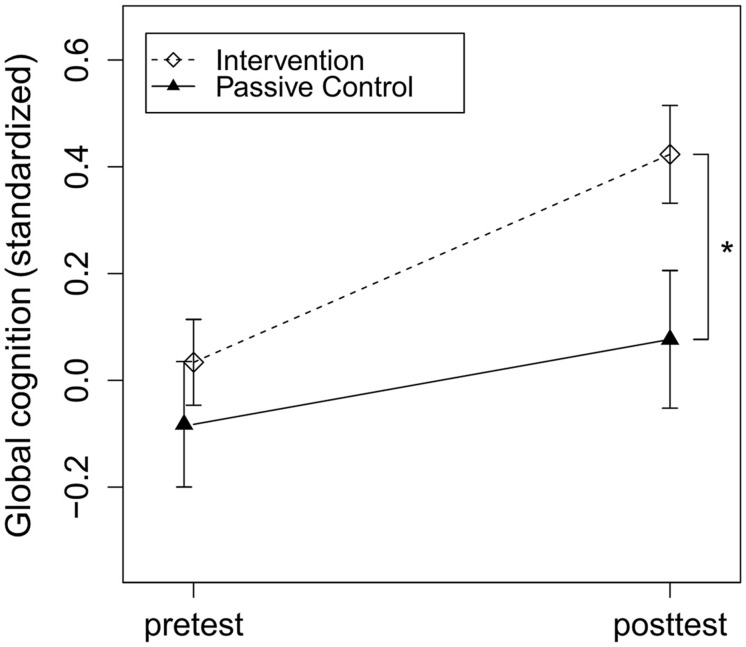
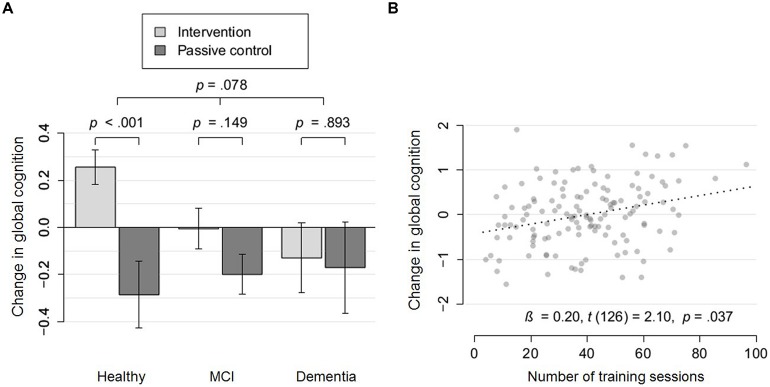
Physical as well as cognitive training interventions improve specific cognitive functions but effects barely generalize on global cognition. Combined physical and cognitive training may overcome this shortcoming as physical training may facilitate the neuroplastic potential which, in turn, may be guided by cognitive training. This study aimed at investigating the benefits of combined training on global cognition while assessing the effect of training dosage and exploring the role of several potential effect modifiers. In this multi-center study, 322 older adults with or without neurocognitive disorders (NCDs) were allocated to a computerized, game-based, combined physical and cognitive training group (n = 237) or a passive control group (n = 85). Training group participants were allocated to different training dosages ranging from 24 to 110 potential sessions. In a pre-post-test design, global cognition was assessed by averaging standardized performance in working memory, episodic memory and executive function tests. The intervention group increased in global cognition compared to the control group, p = 0.002, Cohen's d = 0.31. Exploratory analysis revealed a trend for less benefits in participants with more severe NCD, p = 0.08 (cognitively healthy: d = 0.54; mild cognitive impairment: d = 0.19; dementia: d = 0.04). In participants without dementia, we found a dose-response effect of the potential number and of the completed number of training sessions on global cognition, p = 0.008 and p = 0.04, respectively. The results indicate that combined physical and cognitive training improves global cognition in a dose-responsive manner but these benefits may be less pronounced in older adults with more severe NCD. The long-lasting impact of combined training on the incidence and trajectory of NCDs in relation to its severity should be assessed in future long-term trials.
Keywords: aging; cognitive training; combined intervention; dementia; exergames; mild cognitive impairment; neurocognitive disorder; physical training.
Figures
References
-
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders. Arlington, VA: American Psychiatric Publishing.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical