

Self-Regulation of Anterior Insula with Real-Time fMRI and Its Behavioral Effects in Obsessive-Compulsive Disorder: A Feasibility Study
- PMID: 26301829
- PMCID: PMC4547706
- DOI: 10.1371/journal.pone.0135872
Self-Regulation of Anterior Insula with Real-Time fMRI and Its Behavioral Effects in Obsessive-Compulsive Disorder: A Feasibility Study
Erratum in
-
Correction: Self-Regulation of Anterior Insula with Real-Time fMRI and Its Behavioral Effects in Obsessive-Compulsive Disorder: A Feasibility Study.PLoS One. 2015 Dec 16;10(12):e0145027. doi: 10.1371/journal.pone.0145027. eCollection 2015. PLoS One. 2015. PMID: 26673608 Free PMC article. No abstract available.
Abstract
Introduction: Obsessive-compulsive disorder (OCD) is a common and chronic condition that can have disabling effects throughout the patient's lifespan. Frequent symptoms among OCD patients include fear of contamination and washing compulsions. Several studies have shown a link between contamination fears, disgust over-reactivity, and insula activation in OCD. In concordance with the role of insula in disgust processing, new neural models based on neuroimaging studies suggest that abnormally high activations of insula could be implicated in OCD psychopathology, at least in the subgroup of patients with contamination fears and washing compulsions.
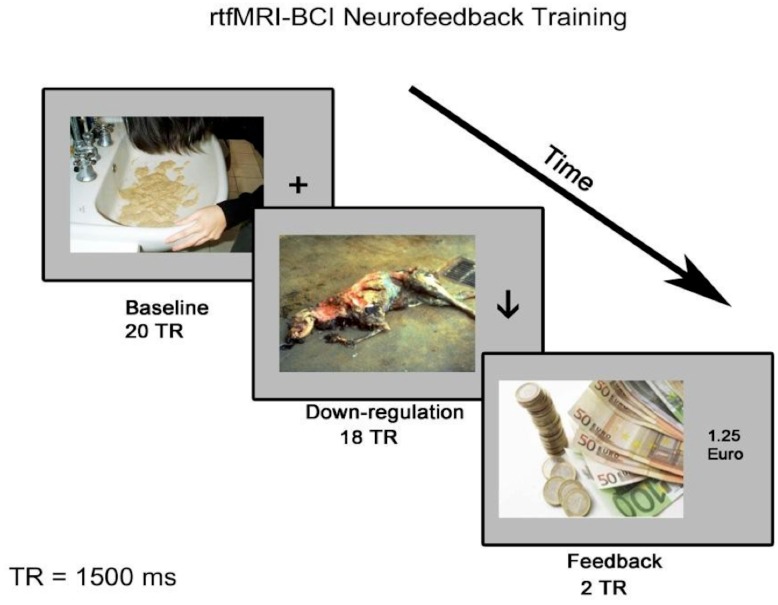
Methods: In the current study, we used a Brain Computer Interface (BCI) based on real-time functional magnetic resonance imaging (rtfMRI) to aid OCD patients to achieve down-regulation of the Blood Oxygenation Level Dependent (BOLD) signal in anterior insula. Our first aim was to investigate whether patients with contamination obsessions and washing compulsions can learn to volitionally decrease (down-regulate) activity in the insula in the presence of disgust/anxiety provoking stimuli. Our second aim was to evaluate the effect of down-regulation on clinical, behavioural and physiological changes pertaining to OCD symptoms. Hence, several pre- and post-training measures were performed, i.e., confronting the patient with a disgust/anxiety inducing real-world object (Ecological Disgust Test), and subjective rating and physiological responses (heart rate, skin conductance level) of disgust towards provoking pictures.
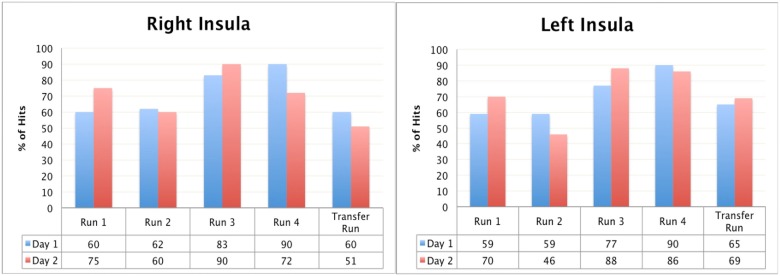
Results: Results of this pilot study, performed in 3 patients (2 females), show that OCD patients can gain self-control of the BOLD activity of insula, albeit to different degrees. In two patients positive changes in behaviour in the EDT were observed following the rtfMRI trainings. Behavioural changes were also confirmed by reductions in the negative valence and in the subjective perception of disgust towards symptom provoking images.
Conclusion: Although preliminary, results of this study confirmed that insula down-regulation is possible in patients suffering from OCD, and that volitional decreases of insula activation could be used for symptom alleviation in this disorder.
Conflict of interest statement
Figures







Similar articles
-
OCD: obsessive-compulsive … disgust? The role of disgust in obsessive-compulsive disorder.J Psychiatry Neurosci. 2017 Sep;42(5):300-306. doi: 10.1503/jpn.160079. J Psychiatry Neurosci. 2017. PMID: 28375077 Free PMC article. Review.
-
Neurocircuitry of disgust and anxiety in obsessive-compulsive disorder: a positron emission tomography study.Metab Brain Dis. 2006 Sep;21(2-3):267-77. doi: 10.1007/s11011-006-9021-6. Epub 2006 Jul 19. Metab Brain Dis. 2006. PMID: 16850255
-
Altered olfactory processing and increased insula activity in patients with obsessive-compulsive disorder: An fMRI study.Psychiatry Res Neuroimaging. 2017 Apr 30;262:15-24. doi: 10.1016/j.pscychresns.2017.01.012. Epub 2017 Feb 9. Psychiatry Res Neuroimaging. 2017. PMID: 28208068 Free PMC article.
-
Neural responses of OCD patients towards disorder-relevant, generally disgust-inducing and fear-inducing pictures.Int J Psychophysiol. 2005 Jul;57(1):69-77. doi: 10.1016/j.ijpsycho.2004.12.013. Epub 2005 Apr 22. Int J Psychophysiol. 2005. PMID: 15935263 Clinical Trial.
-
Disgust and obsessive-compulsive disorder: an update.Psychiatry. 2006 Fall;69(3):228-38. doi: 10.1521/psyc.2006.69.3.228. Psychiatry. 2006. PMID: 17040174 Review.
Cited by
-
OCD: obsessive-compulsive … disgust? The role of disgust in obsessive-compulsive disorder.J Psychiatry Neurosci. 2017 Sep;42(5):300-306. doi: 10.1503/jpn.160079. J Psychiatry Neurosci. 2017. PMID: 28375077 Free PMC article. Review.
-
How feedback, motor imagery, and reward influence brain self-regulation using real-time fMRI.Hum Brain Mapp. 2016 Sep;37(9):3153-71. doi: 10.1002/hbm.23228. Epub 2016 Jun 6. Hum Brain Mapp. 2016. PMID: 27272616 Free PMC article.
-
Real-time functional magnetic resonance imaging in obsessive-compulsive disorder.Neuropsychiatr Dis Treat. 2017 Jul 12;13:1825-1834. doi: 10.2147/NDT.S121139. eCollection 2017. Neuropsychiatr Dis Treat. 2017. PMID: 28744133 Free PMC article. Review.
-
Cognitive and emotional impairments in obsessive-compulsive disorder: Evidence from functional brain alterations.Porto Biomed J. 2016 Jul-Aug;1(3):92-105. doi: 10.1016/j.pbj.2016.07.005. Epub 2016 Jul 1. Porto Biomed J. 2016. PMID: 32258557 Free PMC article. Review.
-
A systematic review of fMRI neurofeedback reporting and effects in clinical populations.Neuroimage Clin. 2020;28:102496. doi: 10.1016/j.nicl.2020.102496. Epub 2020 Nov 11. Neuroimage Clin. 2020. PMID: 33395987 Free PMC article.
References
-
- APA—American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders—DSM-IV-TR (4th edition, Text Revision). Washington, D.C.: American Psychiatric Association; 2000.
-
- Rachman S. Fear of contamination. Behaviour Research and Therapy. 2004; 42(11), 1227–1255. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
