

Beyond Body Mass Index: Advantages of Abdominal Measurements for Recognizing Cardiometabolic Disorders
- PMID: 26302146
- PMCID: PMC5292922
- DOI: 10.1016/j.amjmed.2015.08.010
Beyond Body Mass Index: Advantages of Abdominal Measurements for Recognizing Cardiometabolic Disorders
Abstract
Background: The clinical recognition of cardiometabolic disorders might be enhanced by anthropometry based on the sagittal abdominal diameter (SAD; also called "abdominal height") or waist circumference rather than on weight. Direct comparisons of body mass index (BMI, weight/height(2)) with SAD/height ratio (SADHtR) or waist circumference/height ratio (WHtR) have not previously been tested in nationally representative populations.
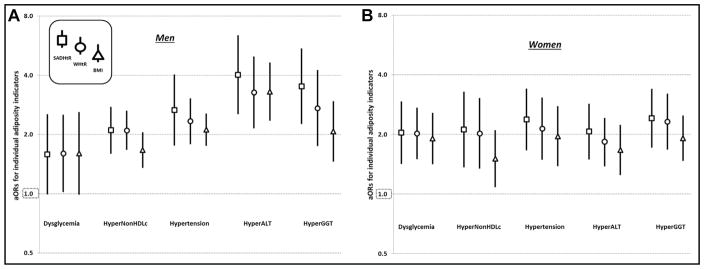
Methods: Nonpregnant adults without diagnosed diabetes (ages 20-64 years; n = 3071) provided conventional anthropometry and supine SAD (by sliding-beam caliper) in the 2011-2012 US National Health and Nutrition Examination Survey. Population-weighted, logistic models estimated how strongly each anthropometric indicator was associated with 5 cardiometabolic disorders: Dysglycemia (glycated hemoglobin ≥5.7%), HyperNonHDLc (non-high-density-lipoprotein [HDL] cholesterol ≥4.14 mmol/L, or taking anticholesteremic medications), Hypertension (systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, or taking antihypertensive medications), HyperALT (alanine transaminase ≥p75 [75th percentile, sex-specific]), and HyperGGT (gamma-glutamyltransferase ≥p75 [sex-specific]).
Results: After scaling each indicator, adjusted odds ratios (aORs) tended to be highest for SADHtR and lowest for BMI when identifying each disorder except dysglycemia. When SADHtR entered models simultaneously with BMI, the aORs for BMI no longer directly identified any condition, whereas SADHtR identified persons with HyperNonHDLc by aOR 2.78 (95% confidence interval [CI], 1.71-4.51), Hypertension by aOR 2.51 (95% CI, 1.22-5.15), HyperALT by aOR 2.89 (95% CI, 1.56-5.37), and HyperGGT by aOR 5.43 (95% CI, 3.01-9.79). WHtR competed successfully against BMI with regard to Dysglycemia, HyperNonHDLc, and HyperGGT. c-Statistics of SADHtR and WHtR were higher than those of BMI (P <.001) for identifying HyperNonHDLc and HyperGGT.
Conclusions: Among nonelderly adults, SADHtR or WHtR recognized cardiometabolic disorders better than did the BMI.
Keywords: Body mass index; Epidemiologic measurements; Hypercholesterolemia; Hypertension; Sagittal abdominal diameter.
Published by Elsevier Inc.
Conflict of interest statement
None.
Figures


Comment in
-
From Leptin, DEXA, and Beyond.Am J Med. 2016 Aug;129(8):e163. doi: 10.1016/j.amjmed.2016.01.052. Am J Med. 2016. PMID: 27453393 No abstract available.
Similar articles
-
Indicators of abdominal size relative to height associated with sex, age, socioeconomic position and ancestry among US adults.PLoS One. 2017 Mar 1;12(3):e0172245. doi: 10.1371/journal.pone.0172245. eCollection 2017. PLoS One. 2017. PMID: 28248983 Free PMC article.
-
Comparison of adiposity indicators associated with fasting-state insulinemia, triglyceridemia, and related risk biomarkers in a nationally representative, adult population.Diabetes Res Clin Pract. 2018 Feb;136:7-15. doi: 10.1016/j.diabres.2017.11.019. Epub 2017 Nov 26. Diabetes Res Clin Pract. 2018. PMID: 29183845 Free PMC article.
-
Population distribution of the sagittal abdominal diameter (SAD) from a representative sample of US adults: comparison of SAD, waist circumference and body mass index for identifying dysglycemia.PLoS One. 2014 Oct 1;9(10):e108707. doi: 10.1371/journal.pone.0108707. eCollection 2014. PLoS One. 2014. PMID: 25272003 Free PMC article.
-
Replacing the body mass index with the sagittal abdominal diameter (abdominal height).Obesity (Silver Spring). 2023 Nov;31(11):2720-2722. doi: 10.1002/oby.23889. Epub 2023 Sep 25. Obesity (Silver Spring). 2023. PMID: 37749805
-
Waist-to-height ratio (WHtR) and triglyceride to HDL-C ratio (TG/HDL-c) as predictors of cardiometabolic risk.Nutr Hosp. 2015 May 1;31(5):2115-21. doi: 10.3305/nh.2015.31.5.7773. Nutr Hosp. 2015. PMID: 25929382
Cited by
-
Milk-Fat Intake and Differences in Abdominal Adiposity and BMI: Evidence Based on 13,544 Randomly-Selected Adults.Nutrients. 2021 May 27;13(6):1832. doi: 10.3390/nu13061832. Nutrients. 2021. PMID: 34072074 Free PMC article.
-
Sagittal Abdominal Diameter, Waist Circumference, and BMI as Predictors of Multiple Measures of Glucose Metabolism: An NHANES Investigation of US Adults.J Diabetes Res. 2018 Jun 19;2018:3604108. doi: 10.1155/2018/3604108. eCollection 2018. J Diabetes Res. 2018. PMID: 30018985 Free PMC article.
-
Dose-response association of obesity and risk of mental health among tehranian residents: result of a cross-sectional study.BMC Public Health. 2024 May 29;24(1):1444. doi: 10.1186/s12889-024-18670-z. BMC Public Health. 2024. PMID: 38811944 Free PMC article.
-
Indicators of abdominal size relative to height associated with sex, age, socioeconomic position and ancestry among US adults.PLoS One. 2017 Mar 1;12(3):e0172245. doi: 10.1371/journal.pone.0172245. eCollection 2017. PLoS One. 2017. PMID: 28248983 Free PMC article.
-
Predictive Validity of the Body Adiposity Index in Overweight and Obese Adults Using Dual-Energy X-ray Absorptiometry.Nutrients. 2016 Nov 30;8(12):737. doi: 10.3390/nu8120737. Nutrients. 2016. PMID: 27916871 Free PMC article.
References
-
- Kuczmarski RJ, Flegal KM. Criteria for definition of overweight in transition: background and recommendations for the United States. Am J Clin Nutr. 2000;72(5):1074–1081. - PubMed
-
- Garn SM, Leonard WR, Hawthorne VM. Three limitations of the body mass index. Am J Clin Nutr. 1986;44(6):996–997. - PubMed
-
- Landsberg L. Body fat distribution and cardiovascular risk: a tale of 2 sites. Arch Intern Med. 2008;168(15):1607–1608. - PubMed
-
- Cornier MA, Despres JP, Davis N, et al. Assessing adiposity: a scientific statement from the American Heart Association. Circulation. 2011;124(18):1996–2019. - PubMed
-
- Rao G, Powell-Wiley TM, Ancheta I, et al. Identification of obesity and cardiovascular risk in ethnically and racially diverse populations: a scientific statement from the American Heart Association. Circulation. 2015;132(5):457–472. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
