

PROMETHEUS: an observational, cross-sectional, retrospective study of hypertriglyceridemia in Russia
- PMID: 26303403
- PMCID: PMC4549018
- DOI: 10.1186/s12933-015-0268-2
PROMETHEUS: an observational, cross-sectional, retrospective study of hypertriglyceridemia in Russia
Abstract
Background: Data regarding the prevalence of hypertriglyceridemia in the Russian population are lacking, despite triglyceride (TG)-mediated pathways being causal in cardiovascular disease. The prevalence of mixed dyslipidemia and severe hypertriglyceridemia in the Russian population (PROMETHEUS) was undertaken to address this gap.
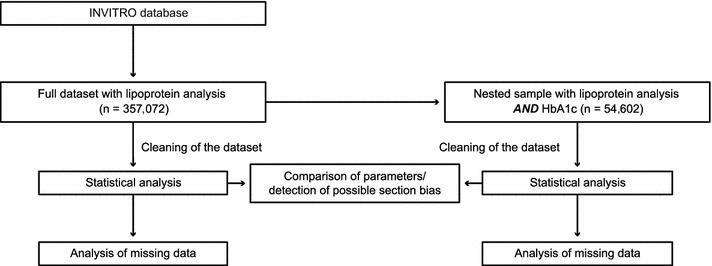
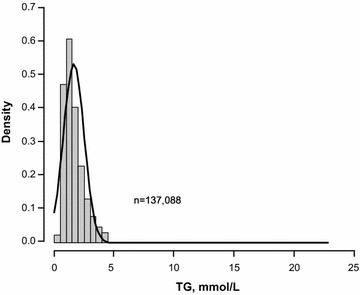
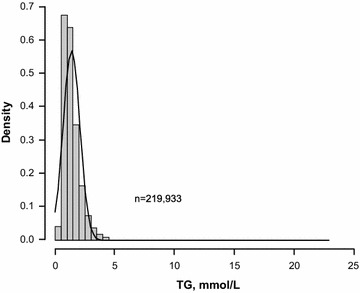
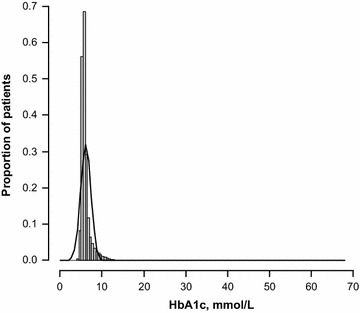
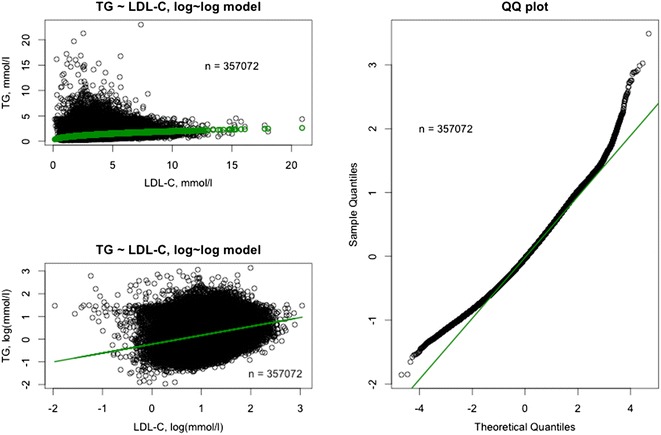
Methods: This was an observational, cross-sectional retrospective study. Data from adults with a full/partial lipoprotein record who had blood analyses done at an INVITRO laboratory in Russia between January 1, 2011 and December 31, 2013 were analyzed. The primary endpoint was the prevalence of hypertriglyceridemia (TG ≥ 1.7 mmol/L); secondary endpoints included prevalence of borderline high, high, and very high TG and severe hypertriglyceridemia, defined as a TG level of 1.7 to <2.3, 2.3 to <5.6, ≥5.6, and ≥10.0 mmol/L, respectively. Statistical analyses involved the Wilcoxon and the Chi square tests. Correlations between log-transformed TG and low- and high-density lipoprotein cholesterol (LDL-C and HDL-C) and total cholesterol (TC) were assessed. The correlation between glycated hemoglobin (HbA1c) and TG levels in a nested sample of subjects with HbA1c and TG data was also assessed using a log-linear model.
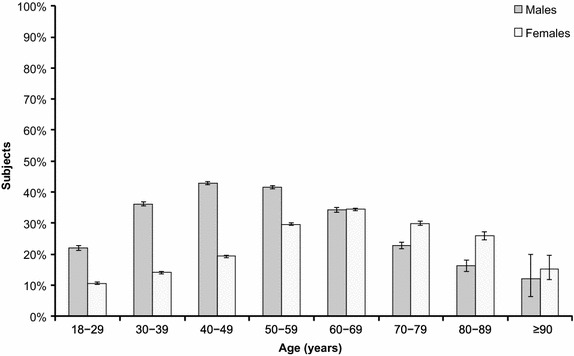
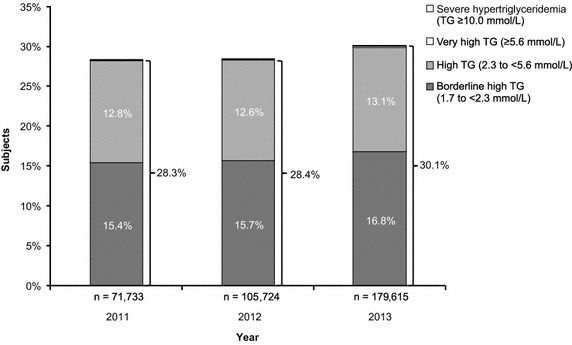
Results: The full dataset and nested sample comprised 357,072 and 54,602 individuals, respectively. Prevalence of hypertriglyceridemia, borderline high TG, high TG, very high TG, and severe hypertriglyceridemia in the full dataset was 29.2, 16.2, 12.9, 0.11, and 0.011%, respectively; corresponding rates in the nested sample were 19.0, 17.2, 0.25, and 0.016%, respectively. TG levels were 16.4% higher in males versus females; males had a greater risk of hypertriglyceridemia (risk ratio 1.25; 95% CI 1.24, 1.26; P < 0.0001). Prevalence of hypertriglyceridemia increased with age, peaking at 40-49 years in males (42.8%) and 60-69 years in females (34.4%); a 0.61% increase in TG levels for each year of life was predicted. Hypertriglyceridemia prevalence increased over time. Correlations between TG and LDL-C, HDL-C, TC, and HbA1c (nested sample only) were observed.
Conclusions: Almost one-third of Russians have hypertriglyceridemia, but severe disease (TG ≥ 10.0 mmol/L) is rare. Although the risk of hypertriglyceridemia was greater in males versus females, its prevalence increased with age, regardless of sex. TG was associated with HbA1c, LDL-C, HDL-C, and TC.
Figures



References
-
- Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration. Sarwar N, Sandhu MS, Ricketts SL, Butterworth AS, Di Angelantonio E, et al. Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010;375:1634–1639. doi: 10.1016/S0140-6736(10)60545-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
