

Association between adverse pregnancy outcome and imbalance in angiogenic regulators and oxidative stress biomarkers in gestational hypertension and preeclampsia
- PMID: 26303772
- PMCID: PMC4549075
- DOI: 10.1186/s12884-015-0624-y
Association between adverse pregnancy outcome and imbalance in angiogenic regulators and oxidative stress biomarkers in gestational hypertension and preeclampsia
Abstract
Background: Gestational hypertension (GH) and Preeclampsia, (PE) are the most complicated amongst hypertensive disorders of pregnancy. The mechanism that links hypertension in pregnancy to adverse maternal outcomes is not fully understood though some relate this to endothelial dysfunction originating from an imbalanced angiogenic regulators and oxidative stress biomarkers. This study assessed the correlation between angiogenic regulators and oxidative stress biomarker levels with adverse pregnancy outcomes among GH and PE participants.
Methods: A cohort of pregnant women who received antenatal care at the Obstetrics and Gynaecology department of the Komfo Anokye Teaching Hospital (KATH) were followed. During their antenatal visits, 100 developed PE and 70 developed GE, of these, 50 PE and 50 GH gave informed consent. Their blood samples were taken at time of diagnosis and 48 h post-partum. 50 other aged-matched women who did not develop neither GH nor PE were selected as controls. Placental growth factor (PLGF), soluble fms-like tyrosine kinase 1 (sFlt-1) and 8-epi-prostaglandin F2alpha (8-epi-PGF2α) levels were estimated by ELISA and total antioxidant capacity (T-AOC) was measured spectrophotometrically. Graphpad Prism was used for data analysis.
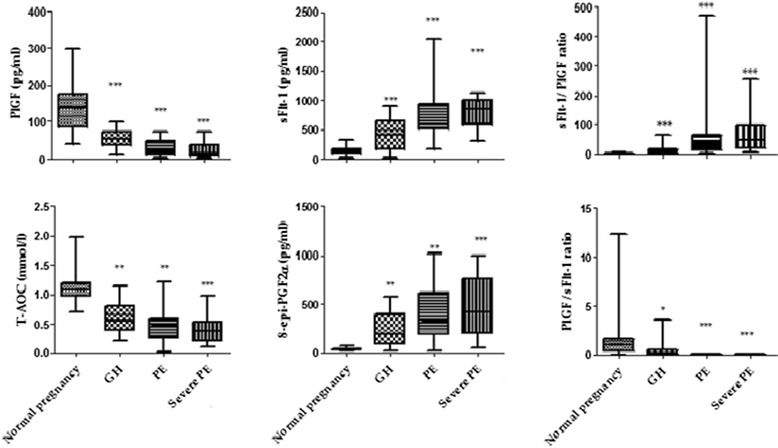
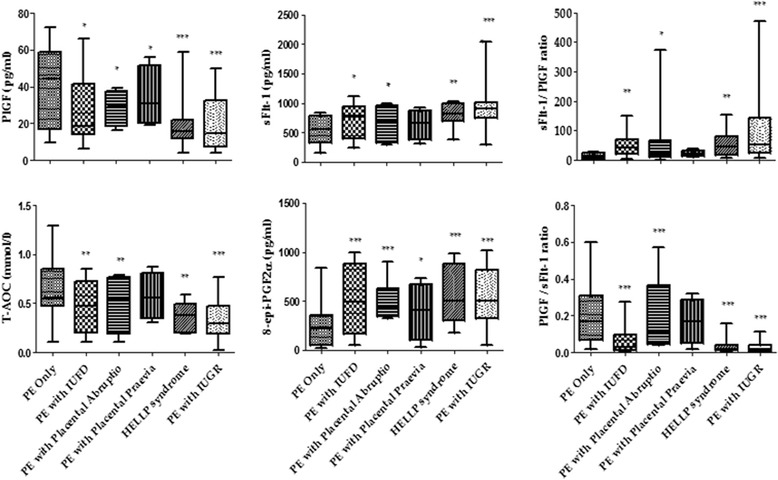
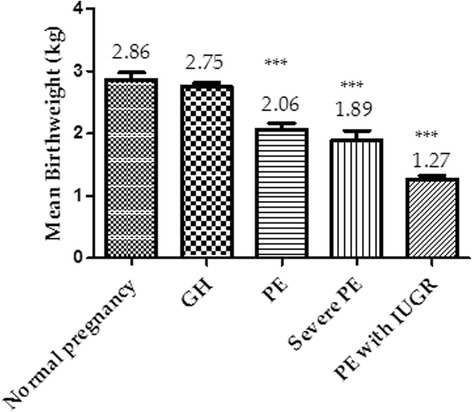
Results: Median levels of sFlt-1, 8-epi-PGF2α and sFlt-1/PLGF were elevated among participants with PE co-existing with intrauterine fetal death (IUFD), placental abruptio, placental previa, HELLP syndrome and intrauterine growth restriction (IUGR) compared to PE without adverse outcomes (p = 0.041, p = 0.005, p = 0.0002). Levels of PLGF, T-AOC and PLGF/sFlt-1 were significantly reduced among participants with PE co-existing with IUFD, placental abruptio, placental previa, HELLP syndrome and IUGR compared to PE without adverse outcomes (p = 0.0013, p = 0.006, p < 0.0001). A significant negative correlation of IUGR (p = 0.0030; p < 0.0001), placental abruptio (p < 0.0001; p < 0.0001), IUFD (p < 0.0001; p < 0.0001), stillbirth (p = 0.0183 and p < 0.000), and postpartum haemorrhage (PPH) (p = 0.0420; p = 0.0044) were associated with both PLGF and T-AOC whilst a significant positive correlation of IUGR, placental abruptio (p < 0.0001; p < 0.0001), IUFD (p < 0.0001; p < 0.0001), stillbirth (p < 0.0001; p < 0.0001), and PPH (p = 0.0043; p = 0.0039) were observed with both sFlt-1 and 8-epi-PGF2α in PE.
Conclusions: Imbalance in the levels of angiogenic regulators and oxidative stress biomarkers correlates with adverse pregnancy outcomes among PE participants. Early identification of these imbalance would alert health care givers in anticipation of adverse pregnancy outcome and thus increased surveillance during pregnancy and parturition and measures to ameliorate the adverse outcome.
Figures
Similar articles
-
Adverse pregnancy outcomes and imbalance in angiogenic growth mediators and oxidative stress biomarkers is associated with advanced maternal age births: A prospective cohort study in Ghana.PLoS One. 2018 Jul 17;13(7):e0200581. doi: 10.1371/journal.pone.0200581. eCollection 2018. PLoS One. 2018. PMID: 30016351 Free PMC article. Clinical Trial.
-
Longitudinal changes in maternal serum placental growth factor and soluble fms-like tyrosine kinase-1 in women at increased risk of pre-eclampsia.Ultrasound Obstet Gynecol. 2016 Mar;47(3):324-31. doi: 10.1002/uog.15750. Epub 2016 Jan 26. Ultrasound Obstet Gynecol. 2016. PMID: 26387758
-
Levels of serum-circulating angiogenic factors within 1 week prior to delivery are closely related to conditions of pregnant women with pre-eclampsia, gestational hypertension, and/or fetal growth restriction.J Obstet Gynaecol Res. 2017 Dec;43(12):1805-1814. doi: 10.1111/jog.13452. Epub 2017 Sep 20. J Obstet Gynaecol Res. 2017. PMID: 28929598
-
Combining Biomarkers to Predict Pregnancy Complications and Redefine Preeclampsia: The Angiogenic-Placental Syndrome.Hypertension. 2020 Apr;75(4):918-926. doi: 10.1161/HYPERTENSIONAHA.119.13763. Epub 2020 Feb 17. Hypertension. 2020. PMID: 32063058 Free PMC article. Review.
-
Clinical utility of sFlt-1 and PlGF in screening, prediction, diagnosis and monitoring of pre-eclampsia and fetal growth restriction.Ultrasound Obstet Gynecol. 2023 Feb;61(2):168-180. doi: 10.1002/uog.26032. Ultrasound Obstet Gynecol. 2023. PMID: 35816445 Review.
Cited by
-
Clinic significance of markedly decreased α-klothoin women with preeclampsia.Am J Transl Res. 2016 May 15;8(5):1998-2010. eCollection 2016. Am J Transl Res. 2016. PMID: 27347309 Free PMC article.
-
Afamin: an early predictor of preeclampsia.Arch Gynecol Obstet. 2018 Nov;298(5):1009-1016. doi: 10.1007/s00404-018-4897-z. Epub 2018 Sep 15. Arch Gynecol Obstet. 2018. PMID: 30220025 Free PMC article.
-
Oxidative stress in pregnancy and reproduction.Obstet Med. 2016 Sep;9(3):113-6. doi: 10.1177/1753495X16648495. Epub 2016 May 17. Obstet Med. 2016. PMID: 27630746 Free PMC article. Review.
-
Effects of Metabolic Syndrome on Pregnancy Outcomes in Women Without Polycystic Ovary Syndrome.J Endocr Soc. 2024 Aug 19;8(10):bvae143. doi: 10.1210/jendso/bvae143. eCollection 2024 Aug 27. J Endocr Soc. 2024. PMID: 39224458 Free PMC article.
-
Fetal programming of human energy homeostasis brain networks: Issues and considerations.Obes Rev. 2022 Mar;23(3):e13392. doi: 10.1111/obr.13392. Epub 2021 Nov 30. Obes Rev. 2022. PMID: 34845821 Free PMC article. Review.
References
-
- Palm M. Oxidative Stress, Angiogenesis and Inflammation in Normal Pregnancy and Postpartum. Acta Universitatis Upsaliensis Digital comprehensive summaries of Uppasala Dissertations from the Faculty of Medicine Uppsala ISBN 978-91-554-8314-2. 2012:753–763.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
