

Risks associated with red blood cell transfusions: potential benefits from application of pathogen inactivation
- PMID: 26303806
- PMCID: PMC7169855
- DOI: 10.1111/trf.13259
Risks associated with red blood cell transfusions: potential benefits from application of pathogen inactivation
Abstract
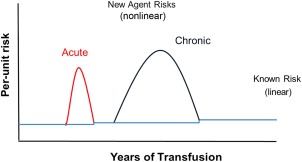
Background: Red blood cell (RBC) transfusion risks could be reduced if a robust technology for pathogen inactivation of RBC (PI-RBCs) were to be approved.
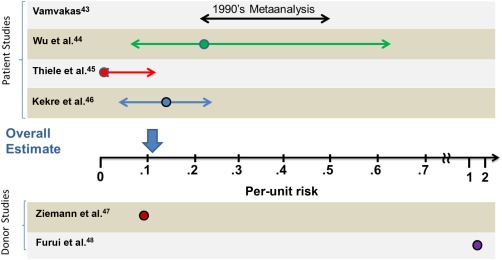
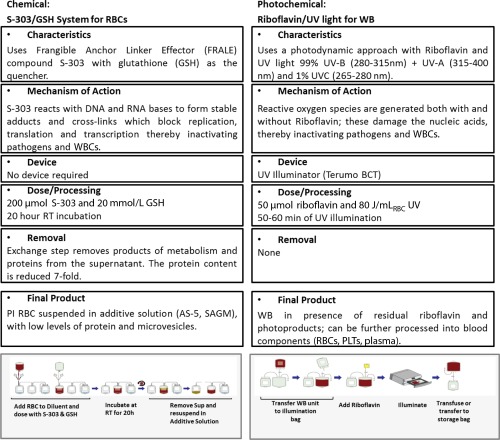
Materials and methods: Estimates of per-unit and per-patient aggregate infectious risks for conventional RBCs were calculated; the latter used patient diagnosis as a determinant of estimated lifetime exposure to RBC units. Existing in vitro data for the two technologies under development for producing PI-RBCs and the status of current clinical trials are reviewed.
Results: Minimum and maximum per-unit risk were calculated as 0.0003% (1 in 323,000) and 0.12% (1 in 831), respectively. The minimum estimate is for known lower-risk pathogens while the maximal estimate also includes an emerging infectious agent (EIA) and endemic area Babesia risk. Minimum and maximum per-patient lifetime risks by diagnosis grouping were estimated as 1.5 and 3.3%, respectively, for stem cell transplantation (which includes additional risk for cytomegalovirus transmission); 1.2 and 3.7%, respectively, for myelodysplastic syndrome; and 0.2 and 44%, respectively, for hemoglobinopathy.
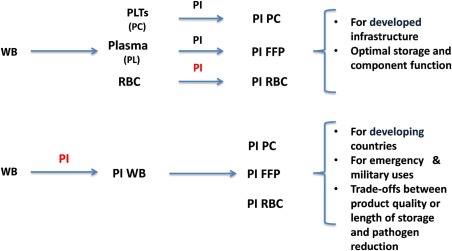
Discussion: There is potential for PI technologies to reduce infectious RBC risk and to provide additional benefits (e.g., prevention of transfusion-associated graft-versus-host disease and possible reduction of alloimmunization) due to white blood cell inactivation. PI-RBCs should be viewed in the context of having a fully PI-treated blood supply, enabling a blood safety paradigm shift from reactive to proactive. Providing insurance against new EIAs. Further, when approved, the use of PI for all components may catalyze operational changes in blood donor screening, laboratory testing, and component manufacturing.
© 2015 AABB.
Conflict of interest statement
SK is a paid consultant to Cerus Corporation; AS is employed by Cerus Corporation.
Figures
References
-
- Kleinman S, Reed W, Stassinopoulos A. A patient‐oriented risk‐benefit analysis of pathogen‐inactivated blood components: application to apheresis platelets in the United States. Transfusion 2013;53:1603‐18. - PubMed
-
- Whitaker B, Hinkins S. The 2011 national blood collection and utilization survey report [Internet]. Washington (DC); US Department of Health and Human Services; 2013 [cited 2014 Dec]. Available from: http://www.hhs.gov/ash/bloodsafety/2011-nbcus.pdf
-
- Kleinman S, Cameron C, Custer B, et al. Modeling the risk of an emerging pathogen entering the Canadian blood supply. Transfusion 2010;50:2592‐606. - PubMed
-
- Custer B, Agapova M, Martinez R. The cost‐effectiveness of pathogen reduction technology as assessed using a multiple risk model. Transfusion 2010;50:2461‐73. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
