

Remote ischaemic preconditioning versus sham procedure for abdominal aortic aneurysm repair: an external feasibility randomized controlled trial
- PMID: 26303818
- PMCID: PMC4549128
- DOI: 10.1186/s13063-015-0899-3
Remote ischaemic preconditioning versus sham procedure for abdominal aortic aneurysm repair: an external feasibility randomized controlled trial
Abstract
Background: Despite advances in perioperative care, elective abdominal aorta aneurysm (AAA) repair carries significant morbidity and mortality. Remote ischaemic preconditioning (RIC) is a physiological phenomenon whereby a brief episode of ischaemia-reperfusion protects against a subsequent longer ischaemic insult. Trials in cardiovascular surgery have shown that RIC can protect patients' organs during surgery. The aim of this study was to investigate whether RIC could be successfully introduced in elective AAA repair and to obtain the information needed to design a multi-centre RCT.
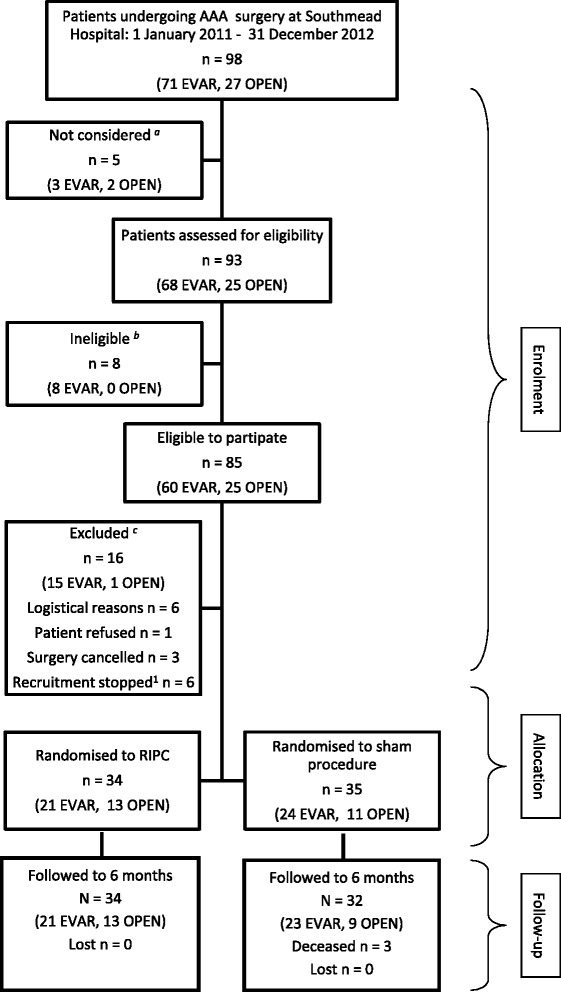
Methods: Consecutive patients presenting for elective AAA repair, using an endovascular (EVAR) or open procedure, in a single large city hospital in the UK were assessed for trial eligibility. Patients who consented to participate were randomized to receive RIC (three cycles of 5 min ischaemia followed by 5 min reperfusion in the upper arm immediately before surgery) or a sham procedure. Patients were followed up for 6 months. We assessed eligibility and consent rates, the logistics of RIC implementation, randomization, blinding, data capture, patient and staff opinion, and variability and frequency of clinical outcome measures.
Results: Between January 2010 and December 2012, 98 patients were referred for AAA repair, 93 were screened, 85 (91%) were eligible, 70 were approached for participation and 69 consented to participate; 34 were randomized to RIC and 35 to the sham procedure. There was a greater than expected variation in the complexity of EVAR that impacted the outcomes. Acute kidney injury occurred in 28 (AKIN 1: 23%; AKIN 2: 15% and AKIN 3: 3%) and 7 (10%) had a perioperative myocardial infarction. Blinding was successful, and interviews with participants and staff indicated that the procedure was acceptable. There were no adverse events secondary to the intervention in the 6 months following the intervention.
Conclusions: This study provided essential information for the planning and design of a multi-centre RCT to assess effectiveness of RIC for improving clinical outcomes in elective AAA repair. Patient consent was high, and the RIC intervention was carried out with minimal disruption to clinical care. The allocation scheme for a definite trial should take into account both the surgical procedure and its complexity to avoid confounding the effect of the RIC, as was observed in this study.
Trial registration: Current Controlled Trials ISRCTN19332276 (date of registration: 16 March 2012). The trial protocol is available from the corresponding author.
Figures
References
-
- Lees S, Taylor P; Stansby G, Patterson B, Baker S, Earnshaw J, et al., National Vascular Database Report, 2009. The Vascular Society of Great Britain and Ireland. http://www.vascularsociety.org.uk/vascular/wpcontent/uploads/2012/11 (accessed August 05, 2013)
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
