

Influence of Baseline Characteristics, Operative Conduct, and Postoperative Course on 30-Day Outcomes of Coronary Artery Bypass Grafting Among Patients With Left Ventricular Dysfunction: Results From the Surgical Treatment for Ischemic Heart Failure (STICH) Trial
- PMID: 26304663
- PMCID: PMC4551105
- DOI: 10.1161/CIRCULATIONAHA.114.014932
Influence of Baseline Characteristics, Operative Conduct, and Postoperative Course on 30-Day Outcomes of Coronary Artery Bypass Grafting Among Patients With Left Ventricular Dysfunction: Results From the Surgical Treatment for Ischemic Heart Failure (STICH) Trial
Abstract
Background: Patients with severe left ventricular dysfunction, ischemic heart failure, and coronary artery disease suitable for coronary artery bypass grafting (CABG) are at higher risk for surgical morbidity and mortality. Paradoxically, those patients with the most severe coronary artery disease and ventricular dysfunction who derive the greatest clinical benefit from CABG are also at the greatest operative risk, which makes decision making regarding whether to proceed to surgery difficult in such patients. To better inform such decision making, we analyzed the Surgical Treatment for Ischemic Heart Failure (STICH) CABG population for detailed information on perioperative risk and outcomes.
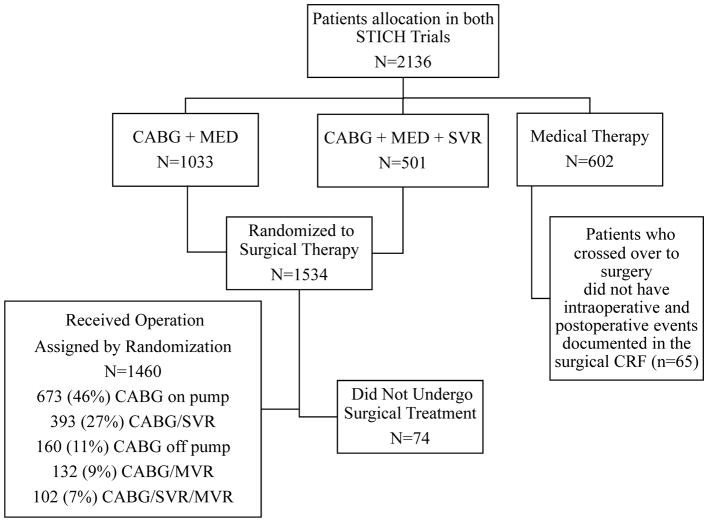
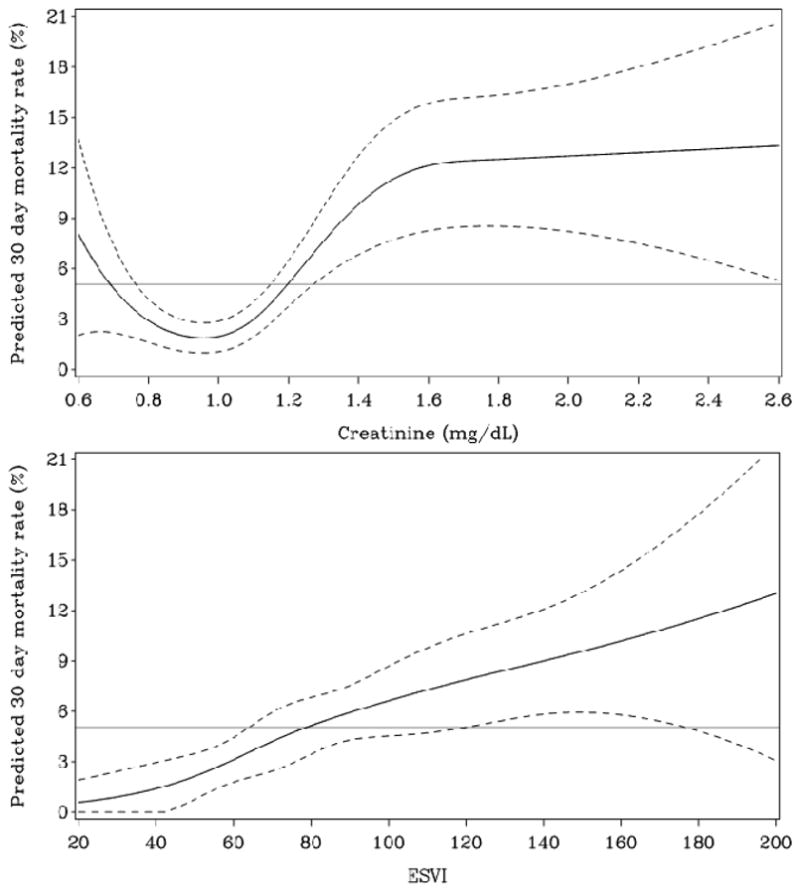
Methods and results: In both STICH trials (hypotheses), 2136 patients with a left ventricular ejection fraction of ≤35% and coronary artery disease were allocated to medical therapy, CABG plus medical therapy, or CABG with surgical ventricular reconstruction. Relationships of baseline characteristics and operative conduct with morbidity and mortality at 30 days were evaluated. There were a total of 1460 patients randomized to and receiving surgery, and 346 (≈25%) of these high-risk patients developed a severe complication within 30 days. Worsening renal insufficiency, cardiac arrest with cardiopulmonary resuscitation, and ventricular arrhythmias were the most frequent complications and those most commonly associated with death. Mortality at 30 days was 5.1% and was generally preceded by a serious complication (65 of 74 deaths). Left ventricular size, renal dysfunction, advanced age, and atrial fibrillation/flutter were significant preoperative predictors of mortality within 30 days. Cardiopulmonary bypass time was the only independent surgical variable predictive of 30-day mortality.
Conclusions: CABG can be performed with relatively low 30-day mortality in patients with left ventricular dysfunction. Serious postoperative complications occurred in nearly 1 in 4 patients and were associated with mortality.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00023595.
Keywords: coronary artery disease; heart failure; myocardial revascularization; surgery.
© 2015 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Panza JA, Velazquez EJ, She L, Smith PK, Nicolau JC, Favaloro RR, Gradinac S, Chrzanowski L, Prabhakaran D, Howlett JG, Jasinski M, Hill JA, Szwed H, Larbalestier R, Desvigne-Nickens P, Jones RH, Lee KL, Rouleau JL. Extent of coronary and myocardial disease and benefit from surgical revascularization in LV dysfunction. J Am Coll Cardiol. 2014;64:553–561. - PMC - PubMed
-
- Shroyer ALW, Coombs LP, Peterson ED, Eiken MC, DeLong ER, Chen A, Ferguson TB, Grover FL, Edwards FH. The Society of Thoracic Surgeons: 30-day operative mortality and morbidity risk models. Ann Thorac Surg. 2003;75:1856–65. discussion 1864–5. - PubMed
-
- Nashef SA, Roques F, Hammill BG, Peterson ED, Michel P, Grover FL, Wyse RK, Ferguson TB. Validation of European System for Cardiac Operative Risk Evaluation (EuroSCORE) in North American cardiac surgery. Eur J Cardiothorac Surg. 2002;22:101–5. - PubMed
-
- Hannan EL, Szypulski Farrell L, Wechsler A, Jordan D, Lahey SJ, Culliford AT, Gold JP, Higgins RSD, Smith CR. The New York risk score for in-hospital and 30-day mortality for coronary artery bypass graft surgery. Ann Thorac Surg. 2013;95:46–54. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
