

Waiting time distribution in public health care: empirics and theory
- PMID: 26304847
- PMCID: PMC4547980
- DOI: 10.1186/s13561-015-0061-7
Waiting time distribution in public health care: empirics and theory
Abstract
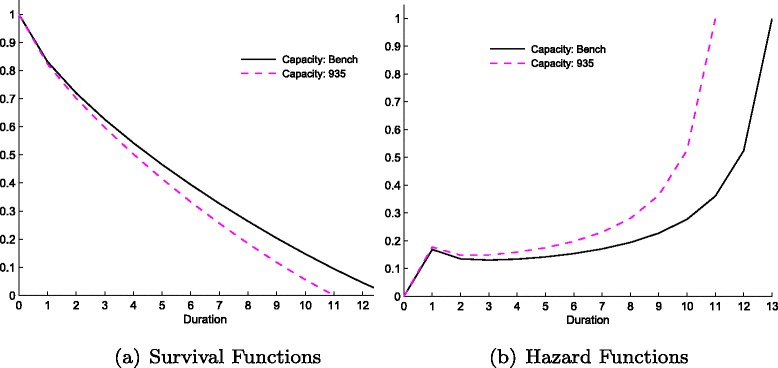
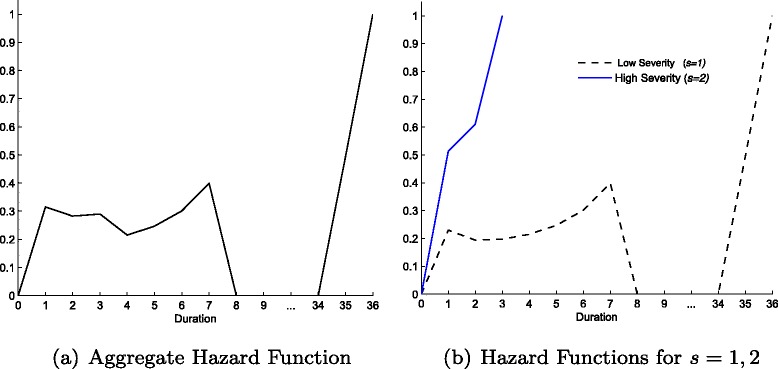
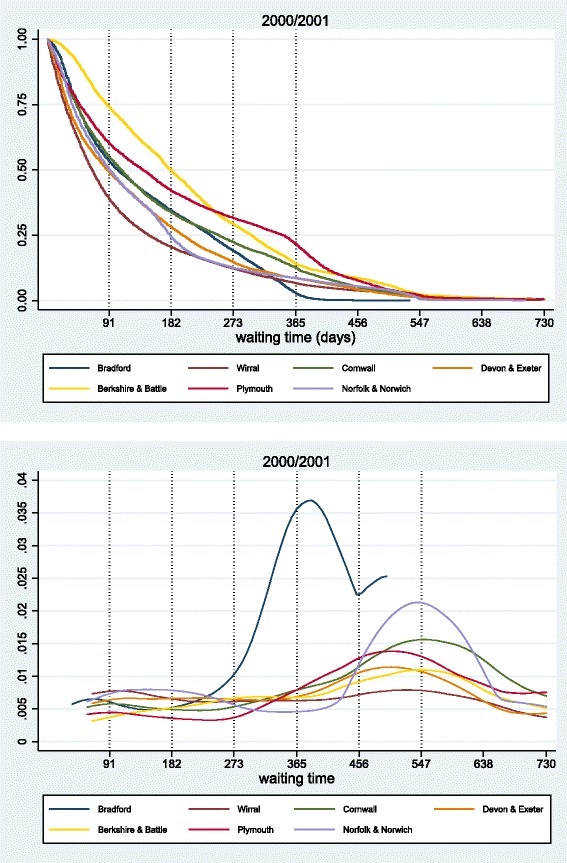
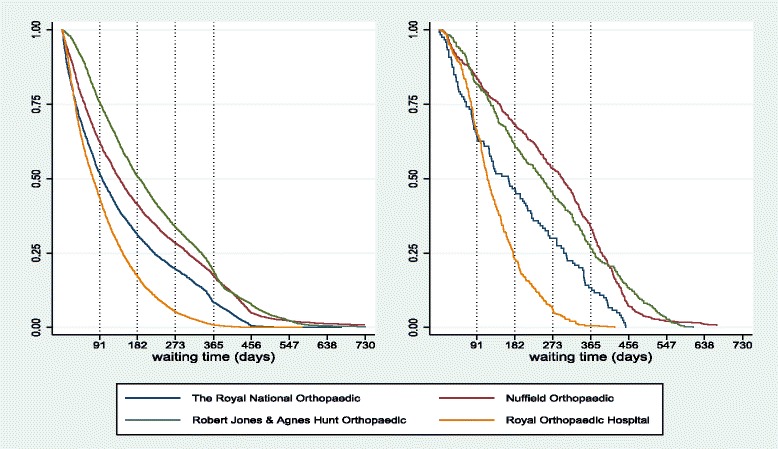
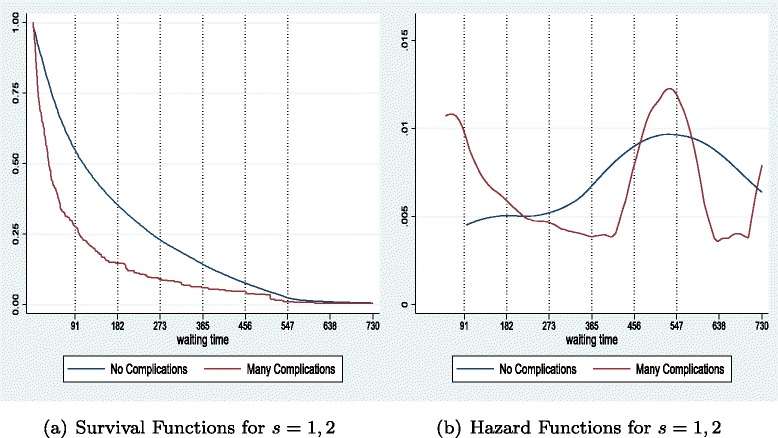
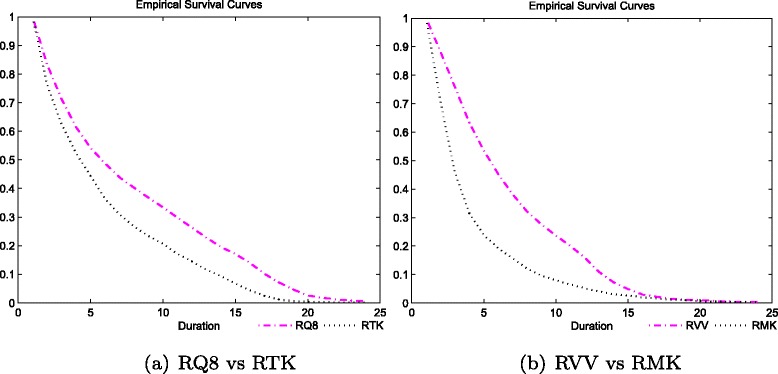
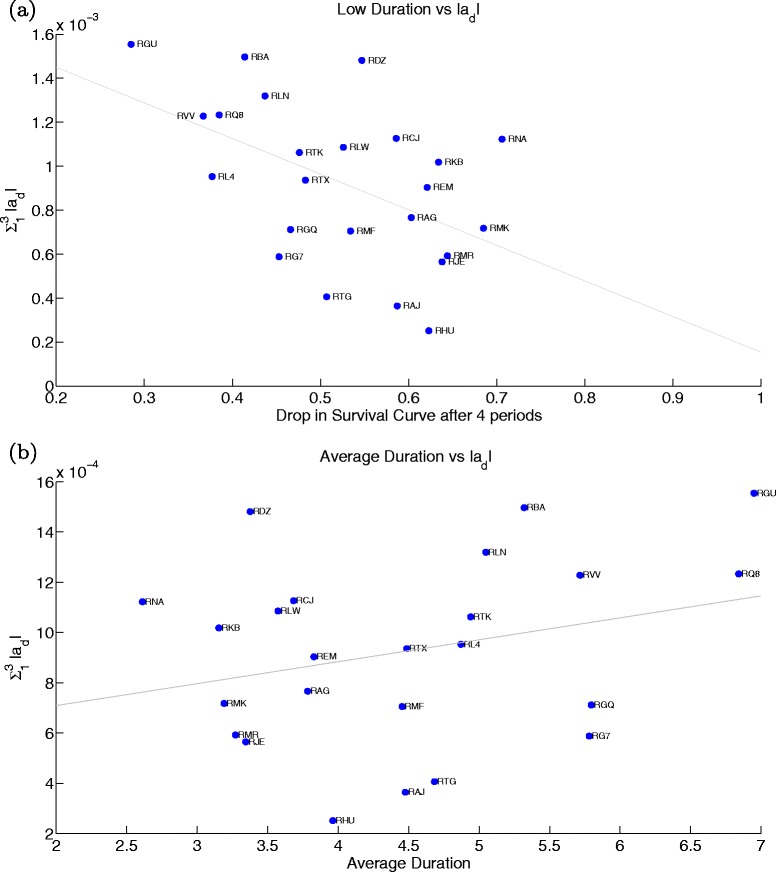
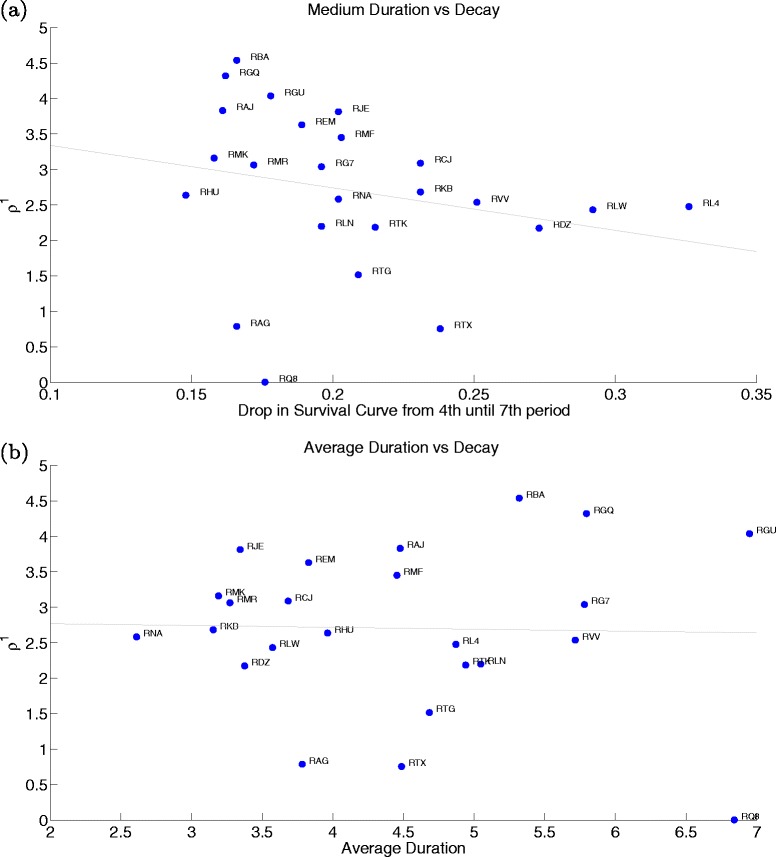
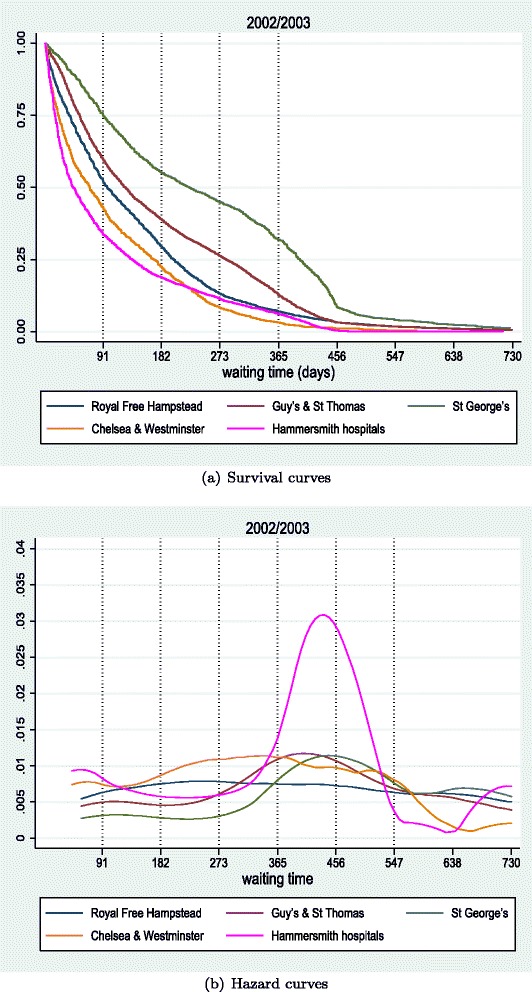
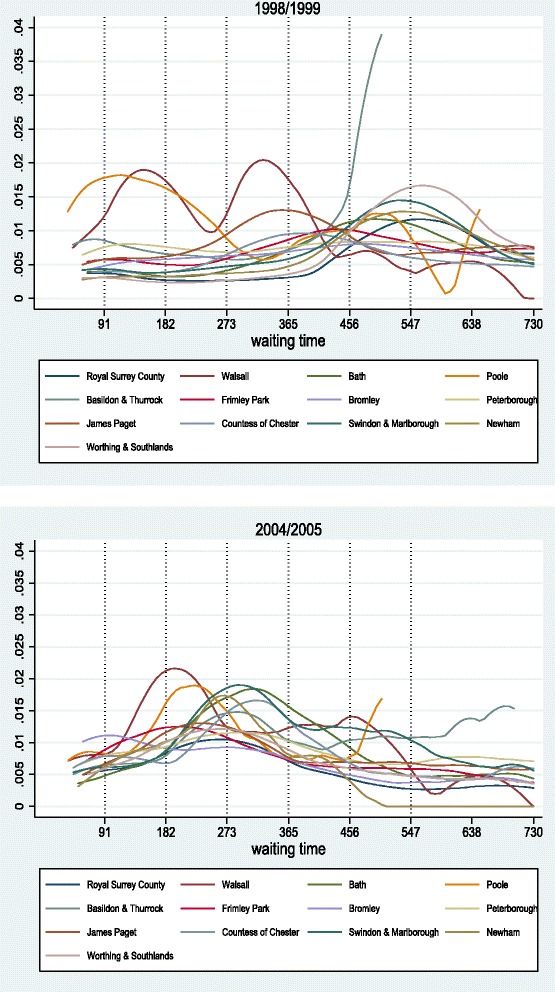
Excessive waiting times for elective surgery have been a long-standing concern in many national healthcare systems in the OECD. How do the hospital admission patterns that generate waiting lists affect different patients? What are the hospitals characteristics that determine waiting times? By developing a model of healthcare provision and analysing empirically the entire waiting time distribution we attempt to shed some light on those issues. We first build a theoretical model that describes the optimal waiting time distribution for capacity constraint hospitals. Secondly, employing duration analysis, we obtain empirical representations of that distribution across hospitals in the UK from 1997-2005. We observe important differences on the 'scale' and on the 'shape' of admission rates. Scale refers to how quickly patients are treated and shape represents trade-offs across duration-treatment profiles. By fitting the theoretical to the empirical distributions we estimate the main structural parameters of the model and are able to closely identify the main drivers of these empirical differences. We find that the level of resources allocated to elective surgery (budget and physical capacity), which determines how constrained the hospital is, explains differences in scale. Changes in benefits and costs structures of healthcare provision, which relate, respectively, to the desire to prioritise patients by duration and the reduction in costs due to delayed treatment, determine the shape, affecting short and long duration patients differently. JEL Classification I11; I18; H51.
Figures








References
LinkOut - more resources
Full Text Sources
Other Literature Sources
