

Non-Vitamin K Antagonist Oral Anticoagulants for Stroke Prevention in Asian Patients With Nonvalvular Atrial Fibrillation: Meta-Analysis
- PMID: 26304863
- PMCID: PMC4542566
- DOI: 10.1161/STROKEAHA.115.009947
Non-Vitamin K Antagonist Oral Anticoagulants for Stroke Prevention in Asian Patients With Nonvalvular Atrial Fibrillation: Meta-Analysis
Abstract
Background and purpose: The use of vitamin K antagonists (VKAs), the cornerstone treatment for stroke prevention in patients with atrial fibrillation, is limited by the perceived risk of serious bleeding in Asia. Non-VKA oral anticoagulants (NOACs) are safer alternatives. Here, we evaluate performance differences of NOACs between Asians and non-Asians.
Methods: We compared efficacy and safety of NOACs between patients enrolled in Asian and non-Asian countries using aggregative data from phase III clinical trials. The odds ratios (ORs [95% confidence interval]) were calculated by a random effects model.
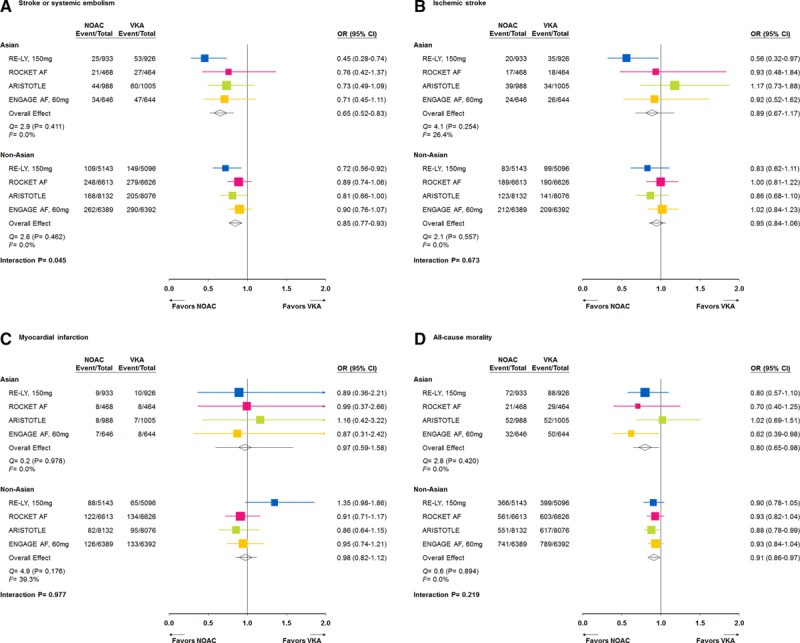
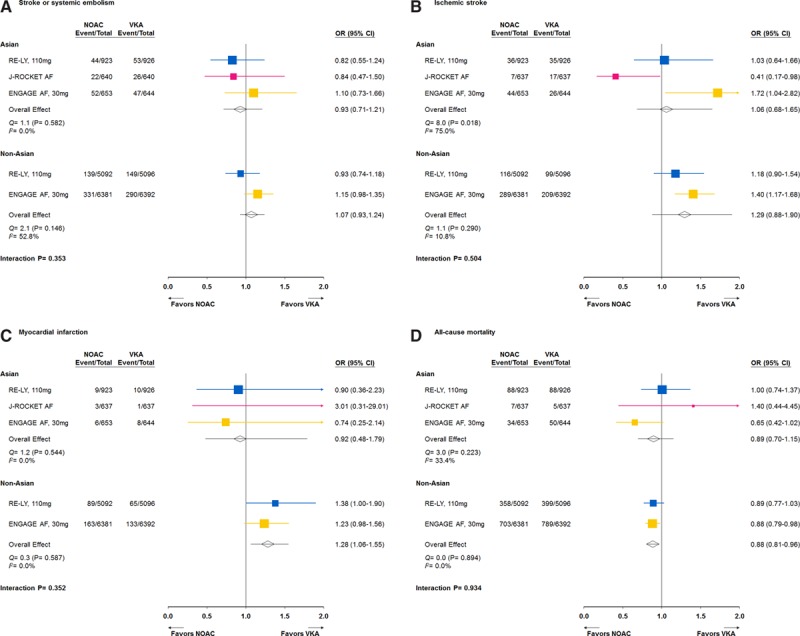
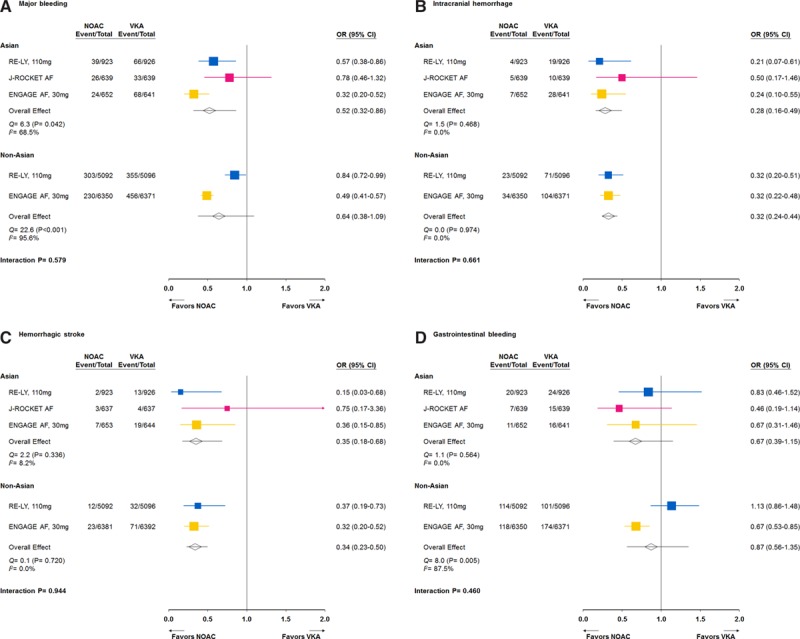
Results: Comparing with VKAs, standard-dose NOACs reduced stroke or systemic embolism (OR=0.65 [0.52-0.83] versus 0.85 [0.77-0.93], P interaction= 0.045) more in Asians than in non-Asians and were safer in Asians than in non-Asians about major bleeding (OR=0.57 [0.44-0.74] versus 0.89 [0.76-1.04], P interaction=0.004), hemorrhagic stroke (OR=0.32 [0.19-0.52] versus 0.56 [0.44-0.70], P interaction=0.046) in particular, whereas gastrointestinal bleeding was significantly increased in non-Asians (OR=0.79 [0.48-1.32] versus 1.44 [1.12-1.85], P interaction=0.041). Generally, low-dose NOACs were safer than VKAs without heterogeneity in efficacy and safety between Asians and non-Asians, except for ischemic stroke, major, and gastrointestinal bleeding.
Conclusions: Our findings suggest that standard-dose NOACs were more effective and safer in Asians than in non-Asians, whereas low-dose NOACs performed similarly in both populations.
Keywords: anticoagulants; atrial fibrillation; hemorrhage; stroke.
© 2015 The Authors.
Figures

References
-
- Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
-
- Shen AY, Yao JF, Brar SS, Jorgensen MB, Chen W. Racial/ethnic differences in the risk of intracranial hemorrhage among patients with atrial fibrillation. J Am Coll Cardiol. 2007;50:309–315. doi: 10.1016/j.jacc.2007.01.098. - PubMed
-
- Gamra H, Murin J, Chiang CE, Naditch-Brûlé L, Brette S, Steg PG RealiseAF investigators. Use of antithrombotics in atrial fibrillation in Africa, Europe, Asia and South America: insights from the International RealiseAF Survey. Arch Cardiovasc Dis. 2014;107:77–87. doi: 10.1016/j.acvd.2014.01.001. - PubMed
-
- Chiang CE, Wang KL, Lip GY. Stroke prevention in atrial fibrillation: an Asian perspective. Thromb Haemost. 2014;111:789–797. doi: 10.1160/TH13-11-0948. - PubMed
-
- Oldgren J, Healey JS, Ezekowitz M, Commerford P, Avezum A, Pais P, et al. RE-LY Atrial Fibrillation Registry Investigators. Variations in cause and management of atrial fibrillation in a prospective registry of 15,400 emergency department patients in 46 countries: the RE-LY Atrial Fibrillation Registry. Circulation. 2014;129:1568–1576. doi: 10.1161/CIRCULATIONAHA.113.005451. - PubMed
