

From Protocols to Publications: A Study in Selective Reporting of Outcomes in Randomized Trials in Oncology
- PMID: 26304898
- PMCID: PMC4979242
- DOI: 10.1200/JCO.2015.62.4148
From Protocols to Publications: A Study in Selective Reporting of Outcomes in Randomized Trials in Oncology
Abstract
Purpose: The decision by journals to append protocols to published reports of randomized trials was a landmark event in clinical trial reporting. However, limited information is available on how this initiative effected transparency and selective reporting of clinical trial data.
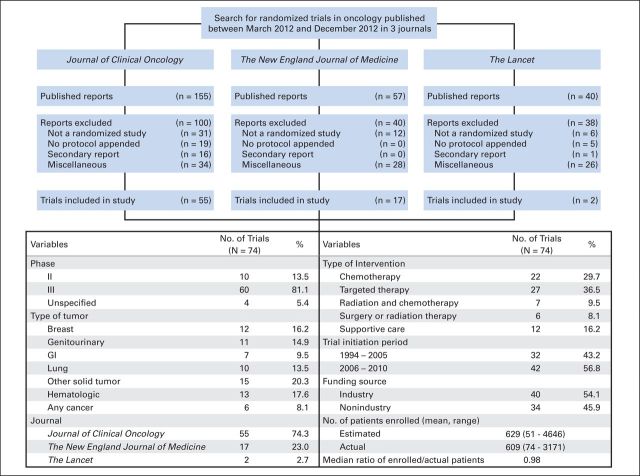
Methods: We analyzed 74 oncology-based randomized trials published in Journal of Clinical Oncology, the New England Journal of Medicine, and The Lancet in 2012. To ascertain integrity of reporting, we compared published reports with their respective appended protocols with regard to primary end points, nonprimary end points, unplanned end points, and unplanned analyses.
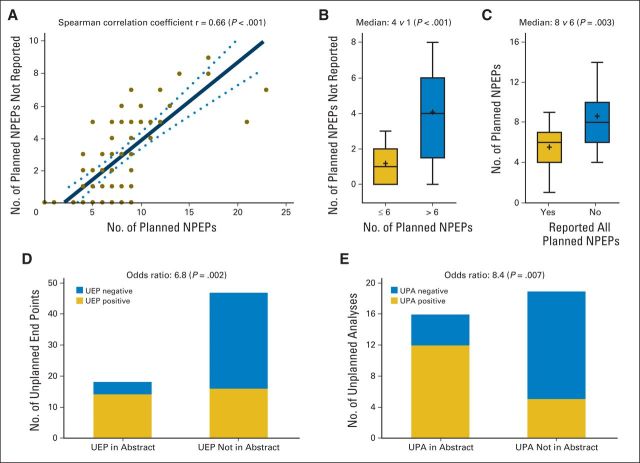
Results: A total of 86 primary end points were reported in 74 randomized trials; nine trials had greater than one primary end point. Nine trials (12.2%) had some discrepancy between their planned and published primary end points. A total of 579 nonprimary end points (median, seven per trial) were planned, of which 373 (64.4%; median, five per trial) were reported. A significant positive correlation was found between the number of planned and nonreported nonprimary end points (Spearman r = 0.66; P < .001). Twenty-eight studies (37.8%) reported a total of 65 unplanned end points; 52 (80.0%) of which were not identified as unplanned. Thirty-one (41.9%) and 19 (25.7%) of 74 trials reported a total of 52 unplanned analyses involving primary end points and 33 unplanned analyses involving nonprimary end points, respectively. Studies reported positive unplanned end points and unplanned analyses more frequently than negative outcomes in abstracts (unplanned end points odds ratio, 6.8; P = .002; unplanned analyses odd ratio, 8.4; P = .007).
Conclusion: Despite public and reviewer access to protocols, selective outcome reporting persists and is a major concern in the reporting of randomized clinical trials. To foster credible evidence-based medicine, additional initiatives are needed to minimize selective reporting.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Similar articles
-
Comparison between publicly accessible publications, registries, and protocols of phase III trials indicated persistence of selective outcome reporting.J Clin Epidemiol. 2017 Nov;91:87-94. doi: 10.1016/j.jclinepi.2017.07.010. Epub 2017 Jul 27. J Clin Epidemiol. 2017. PMID: 28757260 Review.
-
Empirical evidence for selective reporting of outcomes in randomized trials: comparison of protocols to published articles.JAMA. 2004 May 26;291(20):2457-65. doi: 10.1001/jama.291.20.2457. JAMA. 2004. PMID: 15161896
-
Statistical controversies in clinical research: comparison of primary outcomes in protocols, public clinical-trial registries and publications: the example of oncology trials.Ann Oncol. 2017 Apr 1;28(4):688-695. doi: 10.1093/annonc/mdw682. Ann Oncol. 2017. PMID: 28011448
-
Deficiencies in health-related quality-of-life assessment and reporting: a systematic review of oncology randomized phase III trials published between 2012 and 2016.Ann Oncol. 2018 Dec 1;29(12):2288-2295. doi: 10.1093/annonc/mdy449. Ann Oncol. 2018. PMID: 30304498
-
Survival end point reporting in randomized cancer clinical trials: a review of major journals.J Clin Oncol. 2008 Aug 1;26(22):3721-6. doi: 10.1200/JCO.2007.14.1192. J Clin Oncol. 2008. PMID: 18669458 Review.
Cited by
-
Public access to protocols of contemporary cancer randomized clinical trials.Trials. 2021 Jun 27;22(1):418. doi: 10.1186/s13063-021-05382-7. Trials. 2021. PMID: 34176506 Free PMC article.
-
Review and publication of protocol submissions to Trials - what have we learned in 10 years?Trials. 2016 Dec 16;18(1):34. doi: 10.1186/s13063-016-1743-0. Trials. 2016. PMID: 28114958 Free PMC article.
-
Effectiveness of Helicobacter pylori eradication in the prevention of primary gastric cancer in healthy asymptomatic people: A systematic review and meta-analysis comparing risk ratio with risk difference.PLoS One. 2017 Aug 17;12(8):e0183321. doi: 10.1371/journal.pone.0183321. eCollection 2017. PLoS One. 2017. PMID: 28817628 Free PMC article.
-
Risk of Bias and Quality of Reporting in Colon and Rectal Cancer Systematic Reviews Cited by National Comprehensive Cancer Network Guidelines.J Gen Intern Med. 2020 Aug;35(8):2352-2356. doi: 10.1007/s11606-020-05639-y. Epub 2020 Jan 16. J Gen Intern Med. 2020. PMID: 31950401 Free PMC article.
-
Reporting guidelines for oncology research: helping to maximise the impact of your research.Br J Cancer. 2018 Mar 6;118(5):619-628. doi: 10.1038/bjc.2017.407. Epub 2018 Feb 22. Br J Cancer. 2018. PMID: 29471308 Free PMC article. Review.
References
-
- Kirkham JJ, Dwan KM, Altman DG, et al. The impact of outcome reporting bias in randomised controlled trials on a cohort of systematic reviews. BMJ. 2010;340:c365. - PubMed
-
- Franco A, Malhotra N, Simonovits G. Social science: Publication bias in the social sciences—Unlocking the file drawer. Science. 2014;345:1502–1505. - PubMed
-
- Turner EH, Matthews AM, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252–260. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
