

Endogenous Opioid-Masked Latent Pain Sensitization: Studies from Mouse to Human
- PMID: 26305798
- PMCID: PMC4549112
- DOI: 10.1371/journal.pone.0134441
Endogenous Opioid-Masked Latent Pain Sensitization: Studies from Mouse to Human
Abstract
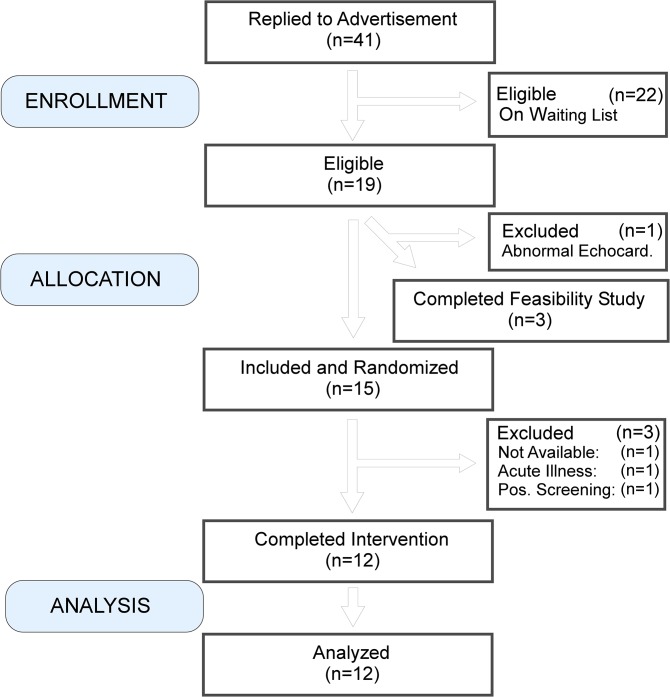
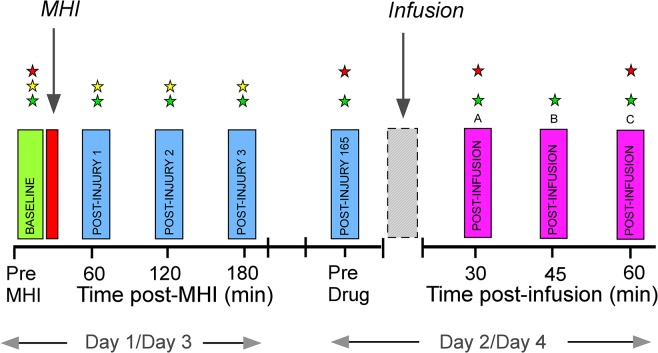
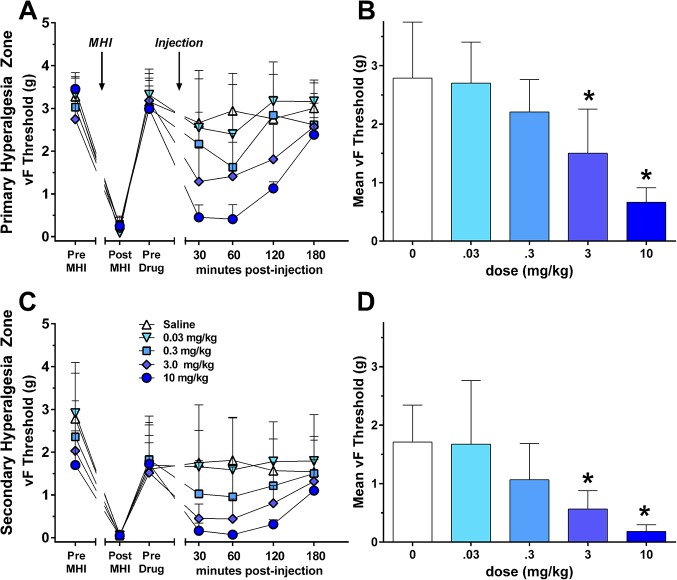
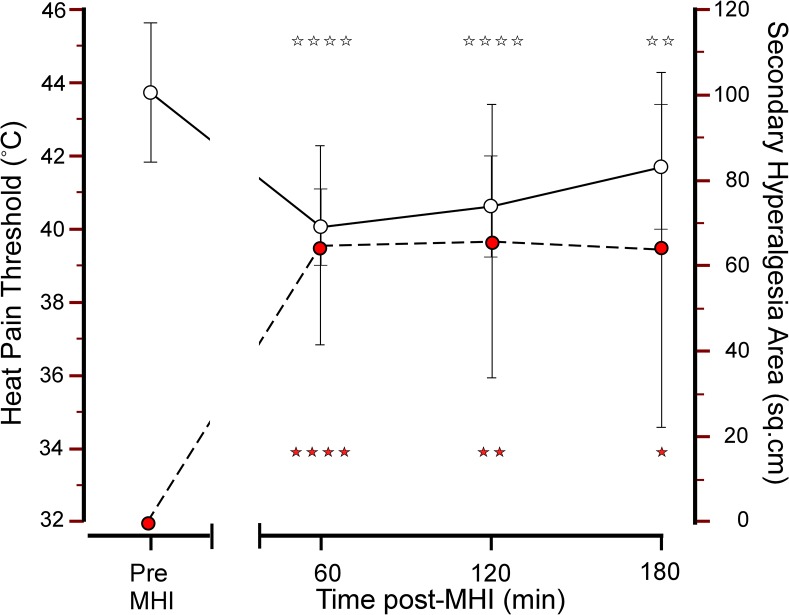
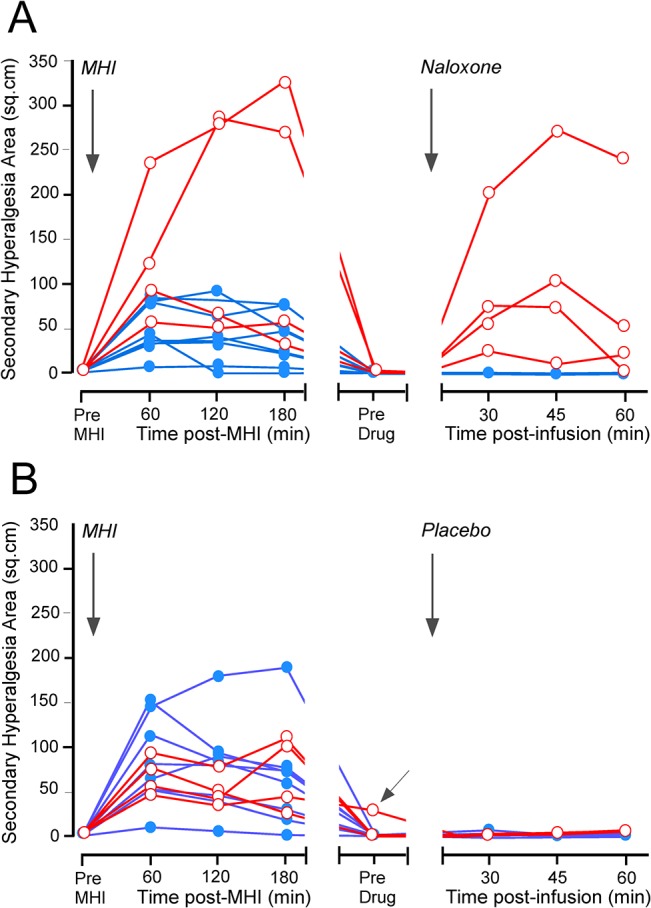
Following the resolution of a severe inflammatory injury in rodents, administration of mu-opioid receptor inverse agonists leads to reinstatement of pain hypersensitivity. The mechanisms underlying this form of latent pain sensitization (LS) likely contribute to the development of chronic pain, but LS has not yet been demonstrated in humans. Using a C57BL/6 mouse model of cutaneous mild heat injury (MHI) we demonstrated a dose-dependent reinstatement of pain sensitization, assessed as primary (P < 0.001) and secondary hyperalgesia (P < 0.001) by naloxone (0.3–10 mg/kg), 168 hrs after the induction of MHI. Forward-translating the dose data to a human MHI model (n = 12) we could show that LS does indeed occur after naloxone 2 mg/kg, 168 hrs after a MHI. Our previous unsuccessful efforts to demonstrate unmasking of LS in humans are thus likely explained by an insufficient naloxone dose (0.021 mg/kg). However, while LS was consistently demonstrated in 21/24 mice, LS was only seen in 4/12 subjects. This difference is likely due to selection bias since the C57BL/6 mouse strain exhibits markedly enhanced pain sensitivity in assays of acute thermal nociception. Future exploratory studies in humans should prioritize inclusion of “high-sensitizers” prone to develop LS and use post-surgical models to elucidate markers of vulnerability to chronic postsurgical pain.
Trial registration: EudraCT 2012-005663-27.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
