

Aging Asian Upper Blepharoplasty and Brow
- PMID: 26306086
- PMCID: PMC4536063
- DOI: 10.1055/s-0035-1556853
Aging Asian Upper Blepharoplasty and Brow
Abstract
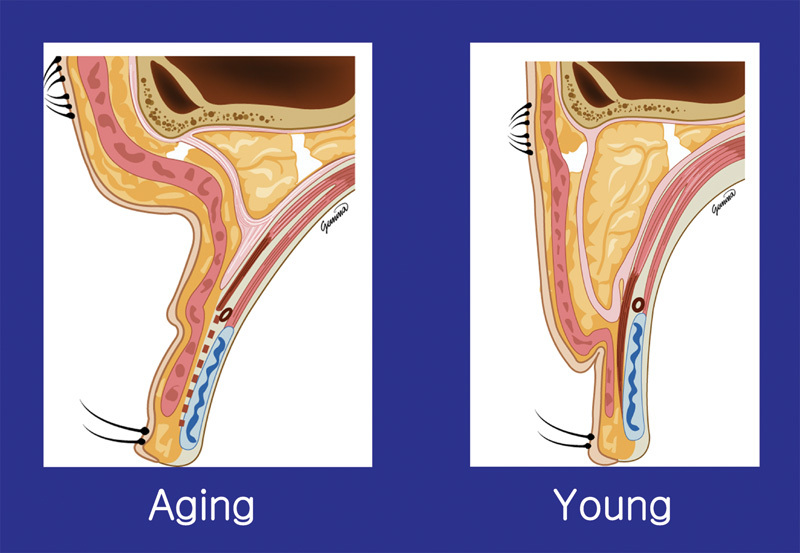
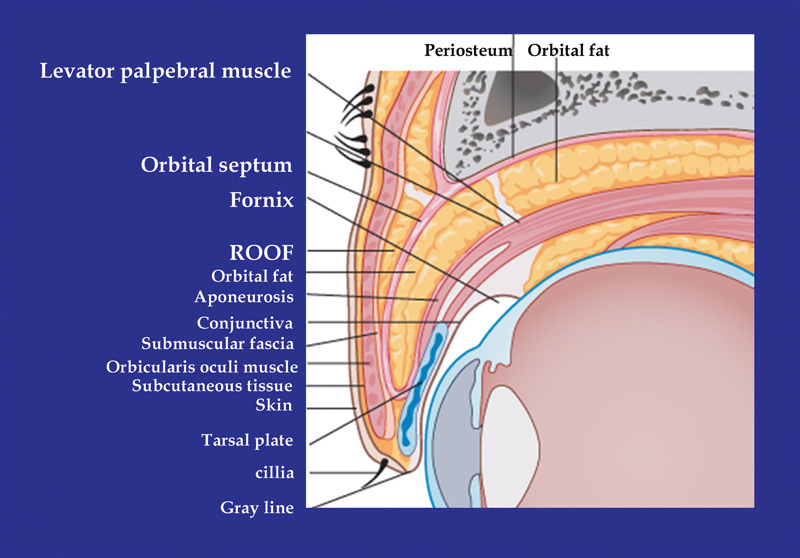
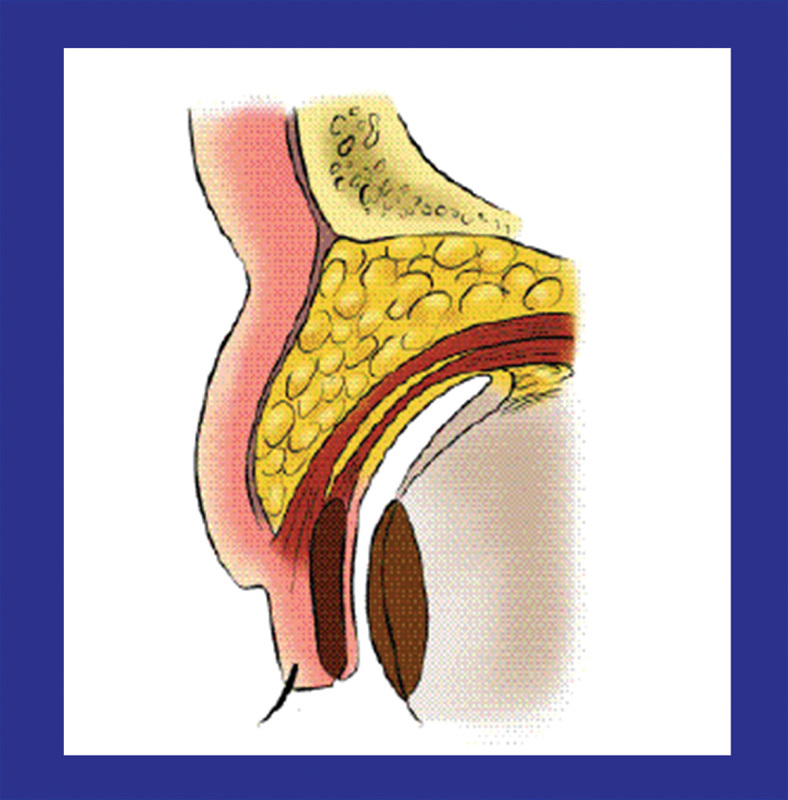
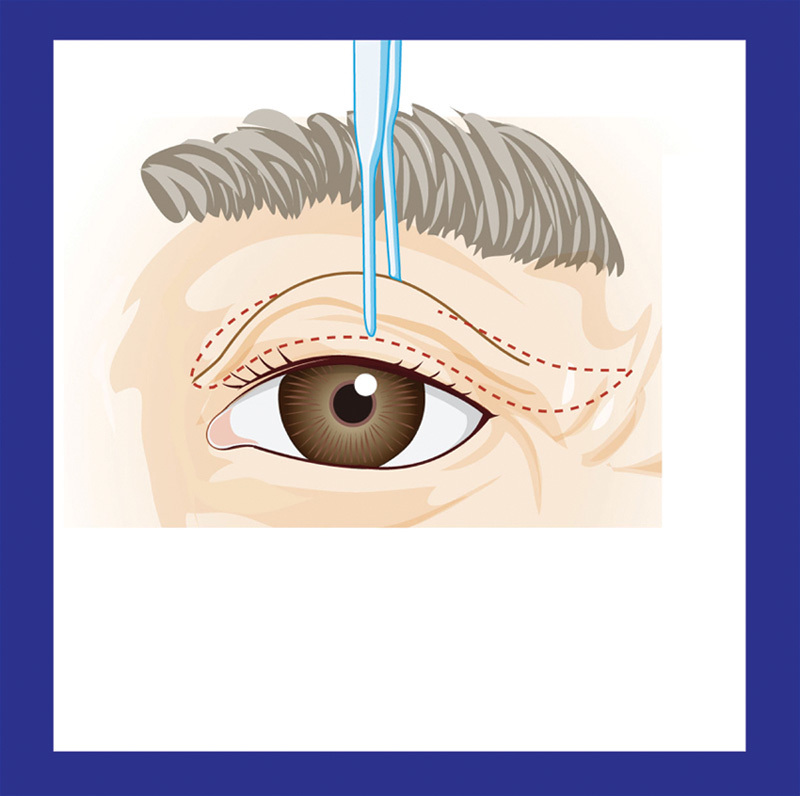
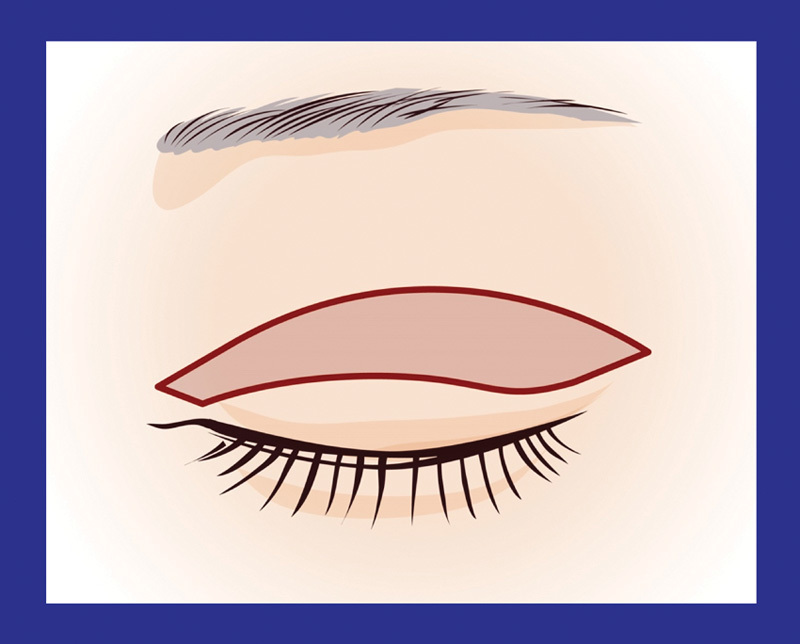
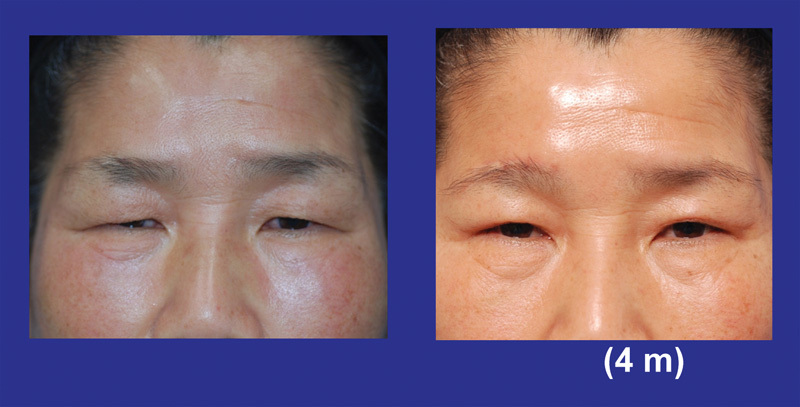
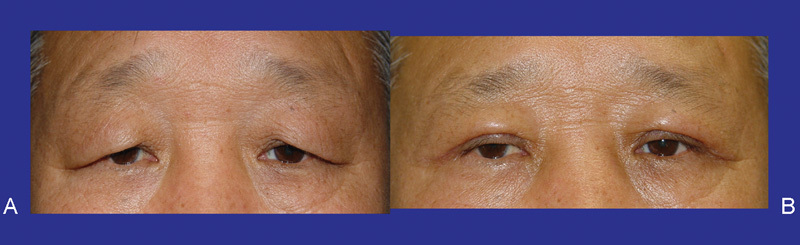
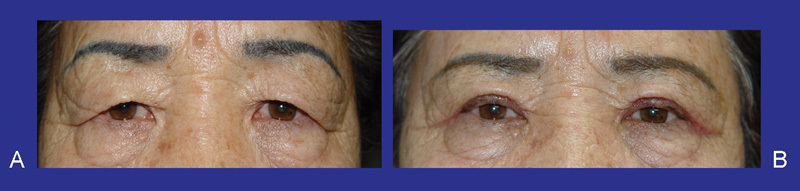
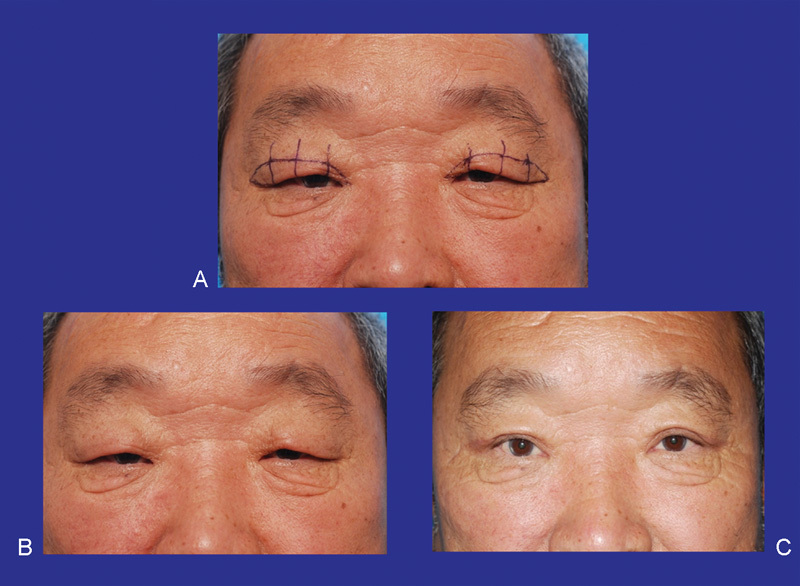
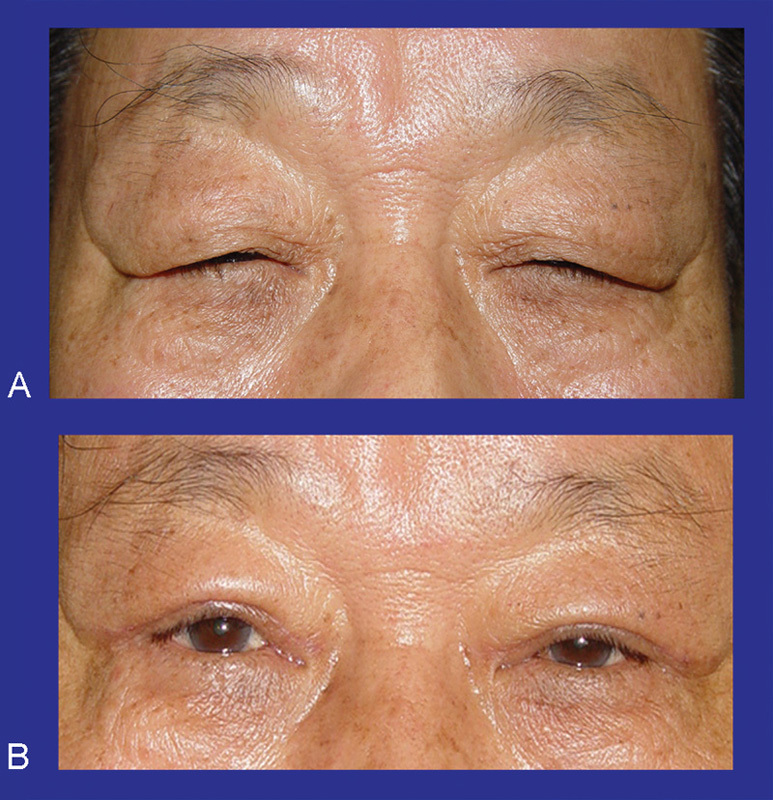
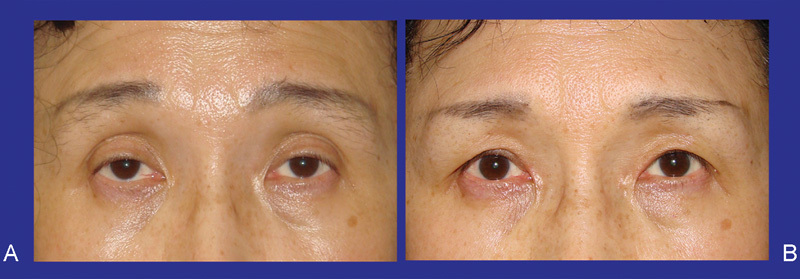
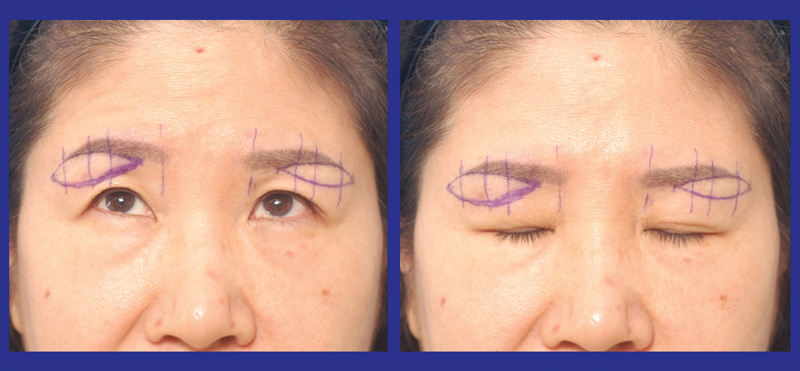
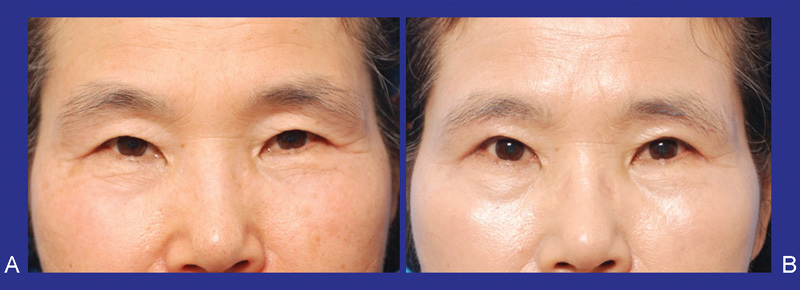
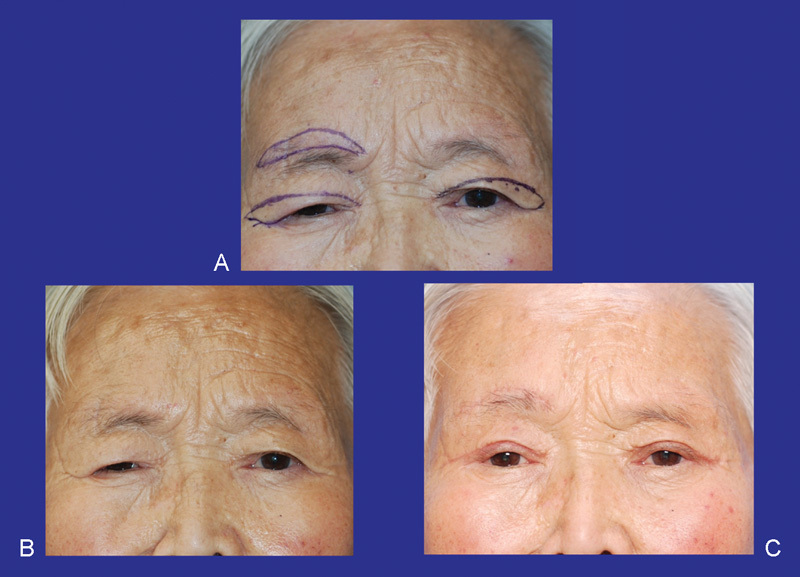
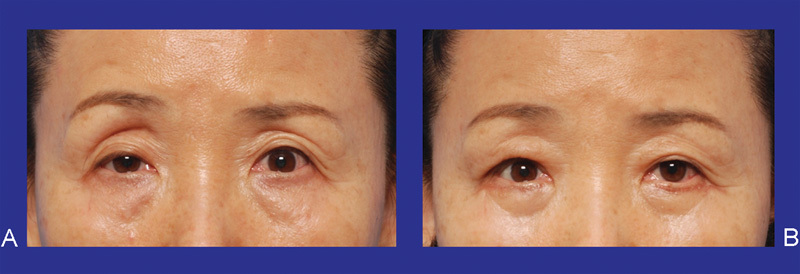
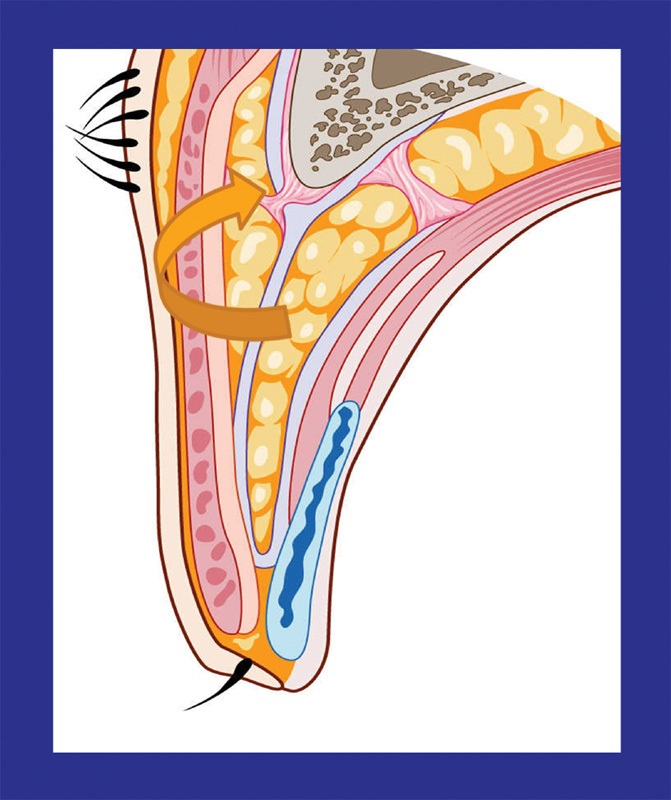
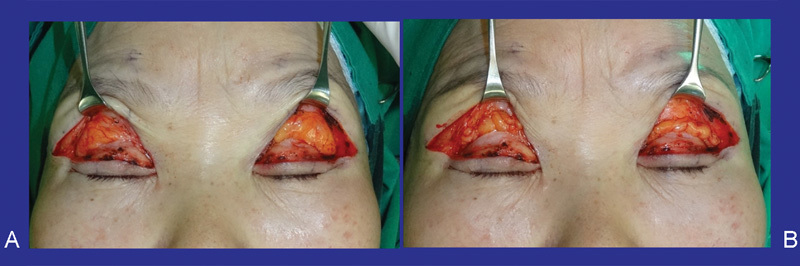
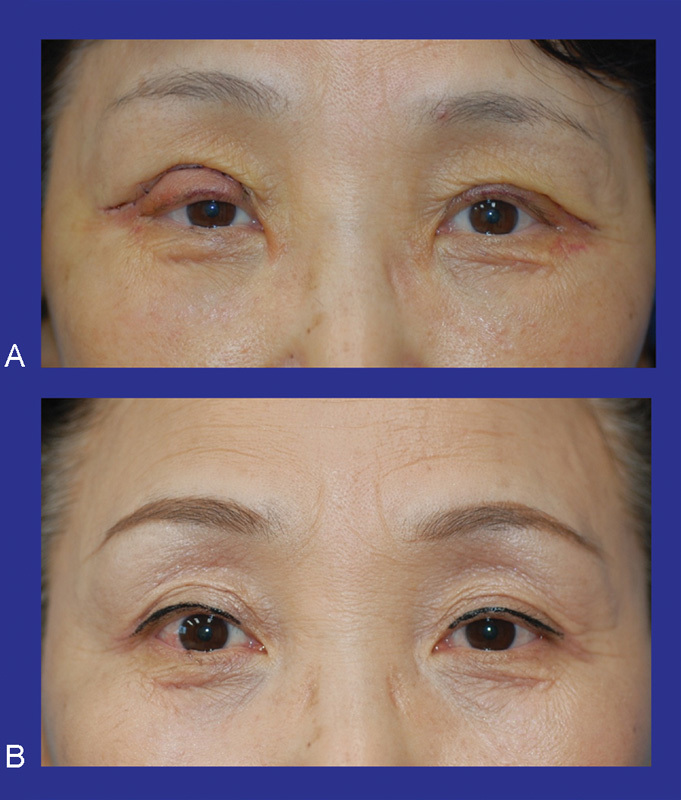
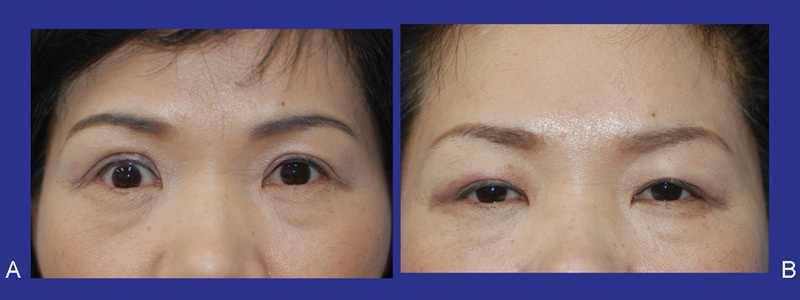
The preoperative comprehensive evaluation of aging Asian patients seeking an Asian upper blepharoplasty and brow lift is imperative and should be performed meticulously. There are many methods of upper Asian face rejuvenation. Among them, the proper selection of operative technique is necessary. The operative technique for an aging Asian upper blepharoplasty and brow lift should be performed based on anatomical structures and their relationship. Modifications to the procedure are correlated with the degree of periorbital aging. The height of double fold in an aging Asian upper blepharoplasty should not exceed 10 mm from the eyelid margin when the eye is closed. The preservation of orbital fat during a blepharoplasty is needed for the prevention of periorbital hollowing, which looks older. For satisfactory results in aging Asian upper blepharoplasty and brow lift, the harmonization of the position of the upper eyelid and eyebrow is important. Noninvasive rejuvenation such as botulinum toxin and filler are good options for facial rejuvenation.
Keywords: Asian blepharoplasty; aging; brow.
Figures


References
-
- Flowers R S, Caputy G G, Flowers S S. The biomechanics of brow and frontalis function and its effect on blepharoplasty. Clin Plast Surg. 1993;20(2):255–268. - PubMed
-
- Flowers R S. Upper blepharoplasty by eyelid invagination. Anchor blepharoplasty. Clin Plast Surg. 1993;20(2):193–207. - PubMed
-
- Dingman D L Transcoronal blepharoplasty Plast Reconstr Surg 1992905815–819., discussion 820 - PubMed
-
- McCord C D, Doxanas M T. Browplasty and browpexy: an adjunct to blepharoplasty. Plast Reconstr Surg. 1990;86(2):248–254. - PubMed
-
- Yun E S, Yun S H, Oh J W, Kim D I. Sub eyebrow skin lifts in persons with tattoos. J Korean Society Aesthet Plast Surg. 1996;2:32.
LinkOut - more resources
Full Text Sources
Other Literature Sources
