

Surgical Ablation of Atrial Fibrillation
- PMID: 26306128
- PMCID: PMC4547665
- DOI: 10.14797/mdcj-11-2-104
Surgical Ablation of Atrial Fibrillation
Abstract
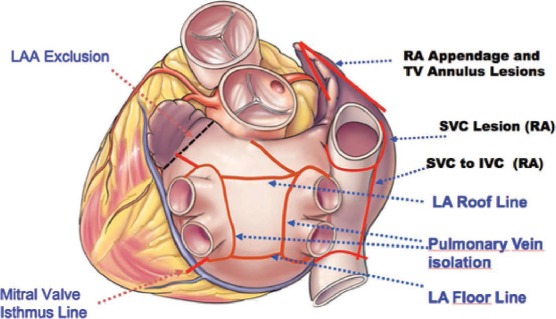
The Cox-maze procedure for the restoration of normal sinus rhythm, initially developed by Dr. James Cox, underwent several iterations over the years. The main concept consists of creating a series of transmural lesions in the right and left atria that disrupt re-entrant circuits responsible for propagating the abnormal atrial fibrillation rhythm. The left atrial appendage is excluded as a component of the Maze procedure. For the first three iterations of the Cox- maze procedure, these lesions were performed using a surgical cut-and-sew approach that ensured transmurality. The Cox-Maze IV is the most currently accepted iteration. It achieves the same lesion set of the Cox- maze III but uses alternative energy sources to create the transmural lesions, potentially in a minimally invasive approach on the beating heart. High-frequency ultrasound, microwave, and laser energy have all been used with varying success in the past. Today, bipolar radiofrequency heat or cryotherapy cooling are the most accepted sources for creating linear lesions with consistent safety and transmurality. The robust and reliable nature of these energy delivery methods has yielded a success rate reaching 90% freedom from atrial fibrillation at 12 months. Such approaches offer a significant long-term advantage over catheter-based ablation, especially in patients having longstanding, persistent atrial fibrillation with characteristics such as dilated left atrial dimensions, poor ejection fraction, and failed catheter ablation. Based on these improved results, there currently is significant interest in developing a hybrid ablation strategy that incorporates the superior transmural robust lesions of surgical ablation, the reliable stroke prevention potential of epicardial left atrial appendage exclusion, and sophisticated mapping and confirmatory catheter-based ablation technology. Such a minimally invasive hybrid strategy for ablation may lead to the development of multidisciplinary "Afib teams" to obtain optimal long-term sinus rhythm control. This article provides an overview of current surgical strategies for patients with atrial fibrillation and addresses the two main goals in its management.
Keywords: atrial fibrillation; maze procedure; surgical ablation.
Figures




Similar articles
-
Surgery for atrial fibrillation.Cardiol Clin. 2014 Nov;32(4):563-71. doi: 10.1016/j.ccl.2014.07.003. Epub 2014 Oct 23. Cardiol Clin. 2014. PMID: 25443237 Free PMC article. Review.
-
Minimally Invasive Stand-Alone Cox Maze Procedure for Persistent and Long-Standing Persistent Atrial Fibrillation: Perioperative Safety and 5-Year Outcomes.Circ Arrhythm Electrophysiol. 2017 Nov;10(11):e005352. doi: 10.1161/CIRCEP.117.005352. Circ Arrhythm Electrophysiol. 2017. PMID: 29138143
-
Surgical ablation for atrial fibrillation for two decades: are the results of new techniques equivalent to the Cox maze III procedure?J Thorac Cardiovasc Surg. 2014 May;147(5):1478-86. doi: 10.1016/j.jtcvs.2013.10.084. Epub 2014 Jan 18. J Thorac Cardiovasc Surg. 2014. PMID: 24560517
-
Current results of minimally invasive surgical ablation for isolated atrial fibrillation.Heart Rhythm. 2009 Dec;6(12 Suppl):S46-9. doi: 10.1016/j.hrthm.2009.08.020. Heart Rhythm. 2009. PMID: 19959143 Review.
-
Catheter Ablation for Long-Standing Persistent Atrial Fibrillation.Methodist Debakey Cardiovasc J. 2015 Apr-Jun;11(2):87-93. doi: 10.14797/mdcj-11-2-87. Methodist Debakey Cardiovasc J. 2015. PMID: 26306125 Free PMC article. Review.
Cited by
-
Efficacy and Safety of Concomitant Surgical Ablation During Mitral Valve Replacement: A Systematic Review.J Saudi Heart Assoc. 2025 Mar 27;37(2):4. doi: 10.37616/2212-5043.1426. eCollection 2025. J Saudi Heart Assoc. 2025. PMID: 40270624 Free PMC article. Review.
-
Comparison between surgical and catheter based ablation in atrial fibrillation, should surgical based ablation be implemented as first line? - A meta-analysis of studies.Indian Pacing Electrophysiol J. 2020 Jan-Feb;20(1):14-20. doi: 10.1016/j.ipej.2019.12.001. Epub 2019 Dec 12. Indian Pacing Electrophysiol J. 2020. PMID: 31838006 Free PMC article.
-
Minimally Invasive Atrial Fibrillation Surgery: Hybrid Approach.Methodist Debakey Cardiovasc J. 2016 Jan-Mar;12(1):37-40. doi: 10.14797/mdcj-12-1-37. Methodist Debakey Cardiovasc J. 2016. PMID: 27127561 Free PMC article. Review.
-
Effects of Modified Simultaneous Unipolar Saline-Irrigated Radiofrequency Ablation in Patients with Atrial Fibrillation Combined with Mitral Valve Disease.Int J Gen Med. 2021 May 26;14:1547-1553. doi: 10.2147/IJGM.S302209. eCollection 2021. Int J Gen Med. 2021. PMID: 34079338 Free PMC article.
-
A Systematic Review on the Effectiveness of Machine Learning in the Detection of Atrial Fibrillation.Curr Cardiol Rev. 2025;21(1):e310724232529. doi: 10.2174/011573403X293703240715104503. Curr Cardiol Rev. 2025. PMID: 39092649 Free PMC article.
References
-
- Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T, Said SA, Darmanata JI, Timmermans AJ, Tijssen JG, Crijns HJ. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med. 2002;347:1834–1840. - PubMed
-
- Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:1825–1833. - PubMed
-
- Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation--pharmacological intervention in atrial fibrillation (piaf): A randomised trial. Lancet. 2000;356:1789–1794. - PubMed
-
- Ad N. The quest to identify predictors for success and failure after the cox-maze procedure for the treatment of atrial fibrillation. J Thorac Cardiovasc Surg. 2010;139:117–118. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
